Teuschl Yvonne, Trapl Michaela, Ratajczak Paulina, Matz Karl, Dachenhausen Alexandra, Brainin Michael
Department for Clinical Neuroscience and Preventive Medicine, Danube University Krems, Krems, Austria.
Department of Neurology, University Hospital Tulln, Tulln, Austria.
PLoS One. 2018 Feb 1;13(2):e0192142. doi: 10.1371/journal.pone.0192142. eCollection 2018.
While formal screening for dysphagia following acute stroke is strongly recommended, there is little evidence on how multi-consistency screening and dietary modifications affect the rate of stroke-associated pneumonia (SAP). This observational study reports which factors affect formal screening on a stroke-unit and how dietary recommendations relate to SAP.
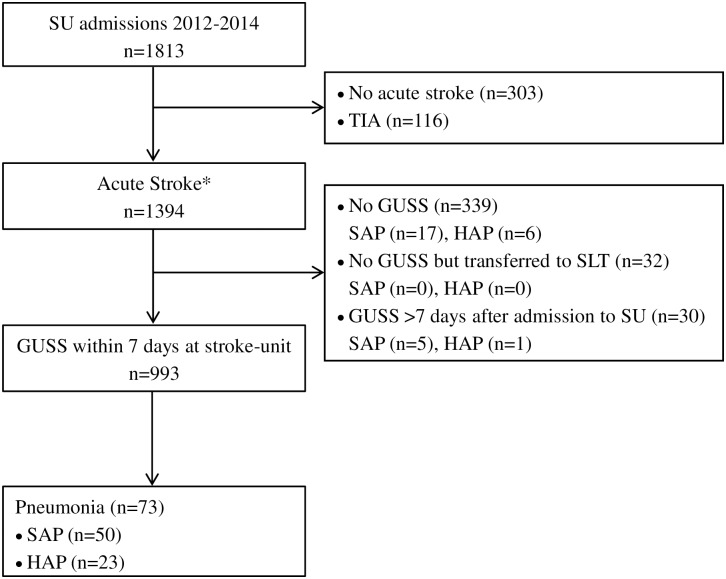
Analyses from a database including 1394 patients admitted with acute stroke at our stroke-unit in Austria between 2012 and 2014. Dietary modifications were performed following the recommendations from the Gugging Swallowing Screen (GUSS). Patients evaluated with GUSS were compared to the unscreened patients.
Overall, 993 (71.2%) patients were screened with GUSS; of these 50 (5.0%) developed SAP. In the 401 unscreened patients, the SAP rate was similar: 22 (5.5%). Multivariable analysis showed that either mild to very mild strokes or very severe strokes were less likely to undergo formal screening. Older age, pre-existing disability, history of hypertension, atrial fibrillation, stroke severity, cardiological and neurological complications, nasogastric tubes, and intubation were significant markers for SAP. Out of 216 patients, 30 (13.9%) developed SAP in spite of receiving nil per mouth (NPO).
The routine use of GUSS is less often applied in either mild strokes or very severe strokes. While most patients with high risk of SAP were identified by GUSS and assigned to NPO, dietary modifications could not prevent SAP in 1 of 7 cases. Other causes of SAP such as silent aspiration, bacteraemia or central breathing disturbances should be considered.
虽然强烈建议对急性卒中后的吞咽困难进行正式筛查,但关于多一致性筛查和饮食调整如何影响卒中相关性肺炎(SAP)发生率的证据很少。这项观察性研究报告了哪些因素影响卒中单元的正式筛查,以及饮食建议与SAP的关系。
对一个数据库进行分析,该数据库包括2012年至2014年期间在奥地利我们的卒中单元收治的1394例急性卒中患者。根据古根吞咽筛查(GUSS)的建议进行饮食调整。将接受GUSS评估的患者与未筛查的患者进行比较。
总体而言,993例(71.2%)患者接受了GUSS筛查;其中50例(5.0%)发生了SAP。在401例未筛查的患者中,SAP发生率相似:22例(5.5%)。多变量分析显示,轻度至非常轻度的卒中或非常严重的卒中接受正式筛查的可能性较小。年龄较大、既往残疾、高血压病史、心房颤动、卒中严重程度、心脏和神经并发症、鼻胃管和插管是SAP的重要标志。在216例患者中,尽管禁食,但仍有30例(13.9%)发生了SAP。
GUSS的常规使用在轻度卒中或非常严重的卒中中较少应用。虽然大多数SAP高危患者通过GUSS被识别并被指定禁食,但饮食调整在7例中有1例无法预防SAP。应考虑SAP的其他原因,如隐性误吸、菌血症或中枢性呼吸障碍。