Kubal Chandrashekhar A, Pennington Catherine, Fridell Jonathan, Ekser Burcin, Muhaylov Plamen, Mangus Richard
Transplant Division, Department of Surgery, Indiana University School of Medicine, Indianapolis, IN, USA.
Department of Pharmacy, Indiana University Health, University Hospital, Indianapolis, IN, USA.
Ann Transplant. 2018 Feb 6;23:98-104. doi: 10.12659/aot.908052.
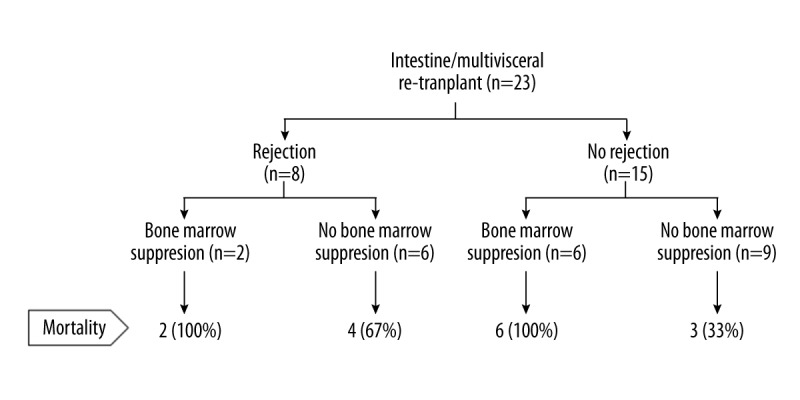
BACKGROUND Patients undergoing re-transplantation often receive high doses of immunosuppression, which may lead to an immunocompromised status of the recipient. This study investigates the outcomes after intestine/multivisceral re-transplantation. MATERIAL AND METHODS Clinical outcomes of 23 patients undergoing 24 re-transplantations at a single intestine transplant center were reviewed. Bone marrow suppression was used as a surrogate marker of immunocompromised status, and was defined as platelet count <50 k/mm3 and absolute lymphocyte count <200/mm³. RESULTS All re-transplants except one were liver inclusive. Fifteen of 23 patients died at a median time of 12 months (range 0.2-75) after re-transplantation. Of the 15 deaths, nine (60%) resulted from complications associated with a compromised host immune status: graft versus host disease (GVHD) affecting bone marrow (three cases), persistent viral infection (three cases), post-transplant lymphoproliferative disorder (PTLD (one case), metastatic cancer (one case), multi-drug resistant polymicrobial sepsis (one case). Four deaths (27%) resulted from severe rejection. Non-survivors were more likely to have received alemtuzumab, and had higher incidence of bone marrow suppression. In addition to immunocompromised status and rejection, the use of alemtuzumab was associated with mortality after intestinal/multivisceral re-transplantation. CONCLUSIONS High mortality was associated with intestine/multivisceral re-transplantation. To improve clinical outcomes of intestine and multivisceral transplantation, it is important to allow reconstitution of host immunity. Longer interval between the two transplantations, and strategies such as allograft specific immunosuppression, may spare the host from the devastating effects of potent immunosuppression currently used.
接受再次移植的患者通常会接受高剂量的免疫抑制治疗,这可能导致受者免疫功能低下。本研究调查了肠道/多脏器再次移植后的结局。
回顾了在单个肠道移植中心接受24次再次移植的23例患者的临床结局。骨髓抑制被用作免疫功能低下状态的替代指标,定义为血小板计数<50 k/mm³和绝对淋巴细胞计数<200/mm³。
除1例再次移植外,所有再次移植均包括肝脏移植。23例患者中有15例在再次移植后中位时间12个月(范围0.2 - 75个月)死亡。在这15例死亡病例中,9例(60%)是由与宿主免疫状态受损相关的并发症导致的:影响骨髓的移植物抗宿主病(GVHD)(3例)、持续性病毒感染(3例)、移植后淋巴细胞增殖性疾病(PTLD)(1例)、转移性癌症(1例)、多重耐药性多微生物败血症(1例)。4例死亡(27%)是由严重排斥反应导致的。非存活者更有可能接受了阿仑单抗治疗,且骨髓抑制发生率更高。除了免疫功能低下状态和排斥反应外,阿仑单抗的使用与肠道/多脏器再次移植后的死亡率相关。
肠道/多脏器再次移植与高死亡率相关。为改善肠道和多脏器移植的临床结局,使宿主免疫功能得以重建非常重要。两次移植之间更长的间隔时间以及同种异体移植特异性免疫抑制等策略,可能使宿主免受目前使用的强效免疫抑制带来的毁灭性影响。