Mansfield Kathryn E, Douglas Ian J, Nitsch Dorothea, Thomas Sara L, Smeeth Liam, Tomlinson Laurie A
Department of Non-Communicable Disease Epidemiology.
Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK.
Clin Epidemiol. 2018 Jan 30;10:187-202. doi: 10.2147/CLEP.S146757. eCollection 2018.
The relative risk of acute kidney injury (AKI) following different infections, and whether angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs) modify the risk, is unclear. We aimed to determine the risks of hospital admission with AKI following infections (urinary tract infection [UTI], lower respiratory tract infection [LRTI], and gastroenteritis) among users of antihypertensive drugs.
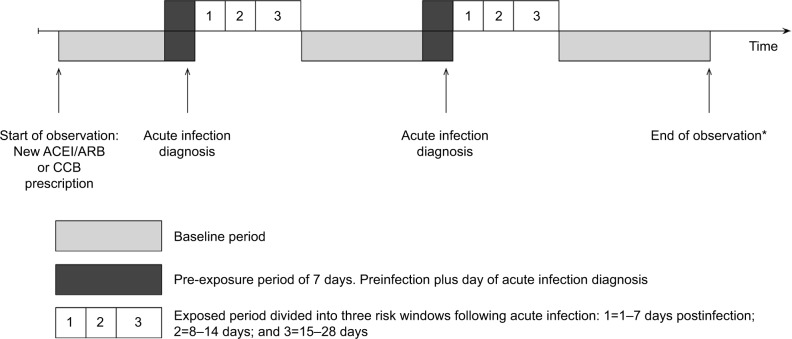
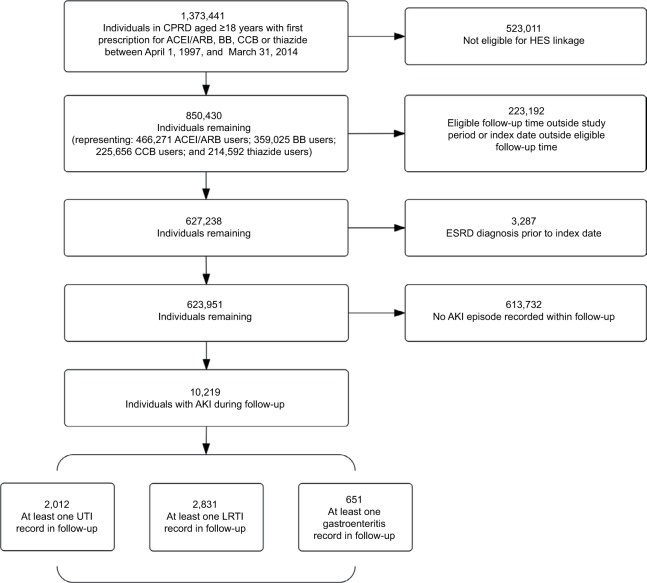
We used UK electronic health records from practices contributing to the Clinical Practice Research Datalink linked to the Hospital Episode Statistics database. We identified adults initiating ACEIs/ARBs or alternative antihypertensive therapy (β-blockers, calcium channel blockers, or thiazide diuretics) between April 1997 and March 2014 with at least 1 year of primary care registration prior to first prescription, who had a hospital admission for AKI, and who had a primary care record for incident UTI, LRTI, or gastroenteritis. We used a self-controlled case series design to calculate age-adjusted incidence rate ratios (IRRs) for AKI during risk periods following acute infection relative to noninfected periods (baseline).
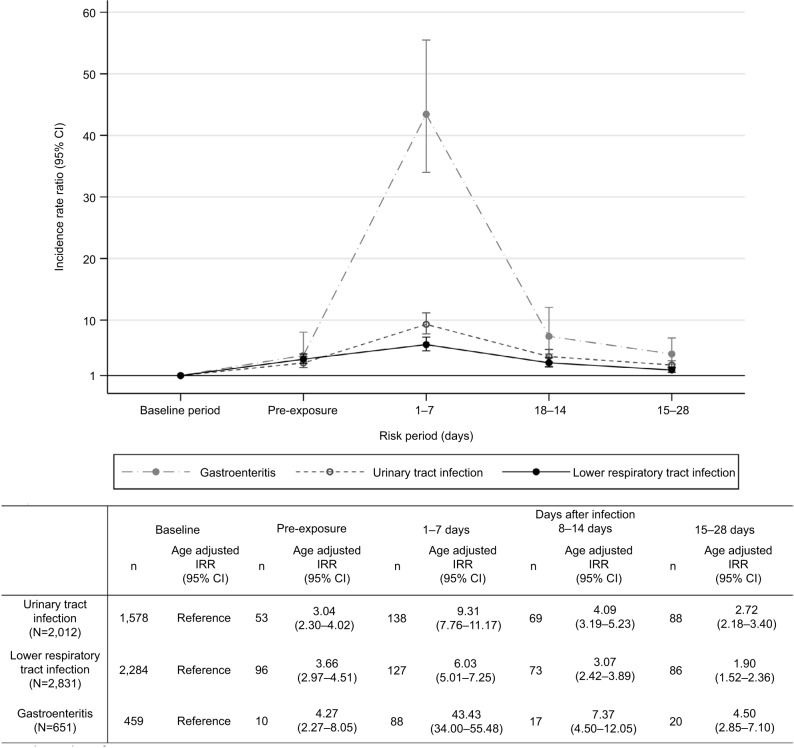
We identified 10,219 eligible new users of ACEIs/ARBs or other antihypertensives with an AKI record. Among these, 2,012 had at least one record for a UTI during follow-up, 2,831 had a record for LRTI, and 651 had a record for gastroenteritis. AKI risk was higher following infection than in baseline noninfectious periods. The rate ratio was highest following gastroenteritis: for the period 1-7 days postinfection, the IRR for AKI following gastroenteritis was 43.4 (95% CI=34.0-55.5), compared with 6.0 following LRTI (95% CI=5.0-7.3), and 9.3 following UTI (95% CI=7.8-11.2). Increased risks were similar for different antihypertensives.
Acute infections are associated with substantially increased transient AKI risk among antihypertensive users, with the highest risk after gastroenteritis. The increase in relative risk is not greater among users of ACEIs/ARBs compared with users of other antihypertensives.
不同感染后发生急性肾损伤(AKI)的相对风险,以及血管紧张素转换酶抑制剂(ACEIs)/血管紧张素受体阻滞剂(ARBs)是否会改变这一风险,目前尚不清楚。我们旨在确定使用抗高血压药物的患者在感染(尿路感染[UTI]、下呼吸道感染[LRTI]和肠胃炎)后因AKI住院的风险。
我们使用了来自参与临床实践研究数据链的医疗机构的英国电子健康记录,该数据链与医院事件统计数据库相关联。我们确定了1997年4月至2014年3月期间开始使用ACEIs/ARBs或其他抗高血压治疗(β受体阻滞剂、钙通道阻滞剂或噻嗪类利尿剂)的成年人,他们在首次处方前至少有1年的初级保健登记记录,因AKI住院,并且有原发性UTI、LRTI或肠胃炎的初级保健记录。我们采用自我对照病例系列设计来计算急性感染后风险期内AKI相对于未感染期(基线)的年龄调整发病率比(IRRs)。
我们确定了10219名符合条件的新使用ACEIs/ARBs或其他抗高血压药物且有AKI记录的患者。其中,2012名患者在随访期间至少有一次UTI记录,2831名患者有LRTI记录,651名患者有肠胃炎记录。感染后的AKI风险高于基线非感染期。肠胃炎后的发病率比最高:感染后1 - 7天内,肠胃炎后AKI的IRR为43.4(95%CI = 34.0 - 55.5),而LRTI后为6.0(95%CI = 5.0 - 7.3),UTI后为9.3(95%CI = 7.8 - 11.2)。不同抗高血压药物的风险增加相似。
急性感染与抗高血压药物使用者中短暂性AKI风险的大幅增加相关,肠胃炎后的风险最高。与其他抗高血压药物使用者相比,ACEIs/ARBs使用者的相对风险增加并不更大。