Yamamoto Takeshi
Division of Cardiovascular Intensive Care, Nippon Medical School Hospital, 1-1-5 Sendagi, Bunkyo-ku, Tokyo, 113-8603 Japan.
J Intensive Care. 2018 Mar 2;6:16. doi: 10.1186/s40560-018-0286-8. eCollection 2018.
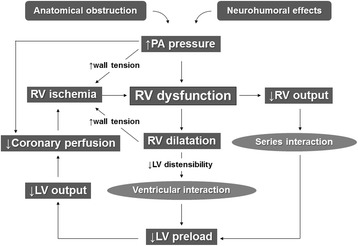
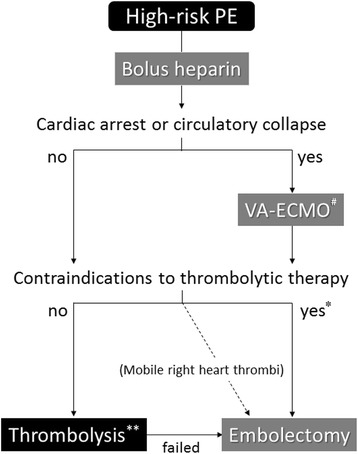
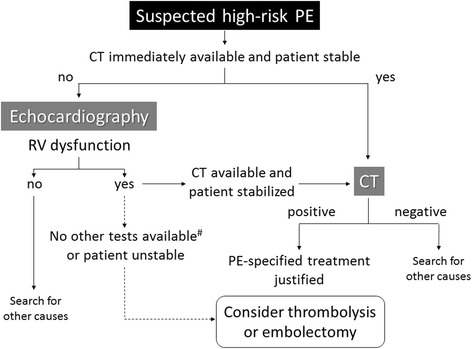
High-risk pulmonary embolism (PE) is a life-threatening disorder associated with high mortality and morbidity. Most deaths in patients with shock occur within the first few hours after presentation, and rapid diagnosis and treatment is therefore essential to save patients' lives. The main manifestations of major PE are acute right ventricular (RV) failure and hypoxia. RV pressure overload is predominantly related to the interaction between the mechanical pulmonary vascular obstruction and the underlying cardiopulmonary status. Computed tomography angiography allows not only adequate visualization of the pulmonary thromboemboli down to at least the segmental level but also RV enlargement as an indicator of RV dysfunction. Bedside echocardiography is an acceptable alternative under such circumstances. Although it does not usually provide a definitive diagnosis or exclude pulmonary embolism, echocardiography can confirm or exclude severe RV pressure overload and dysfunction. Extracorporeal membrane oxygenation support can be an effective procedure in patients with PE-induced circulatory collapse. Thrombolysis is generally accepted in unstable patients with high-risk PE; however, thrombolytic agents cannot be fully administered to patients with a high risk of bleeding. Conversely, catheter-directed treatment is an optimal treatment strategy for patients with high-risk PE who have contraindications for thrombolysis and is a minimally invasive alternative to surgical embolectomy. It can be performed with a minimum dose of thrombolytic agents or without, and it can be combined with various procedures including catheter fragmentation or embolectomy in accordance with the extent of the thrombus on a pulmonary angiogram. Hybrid catheter-directed treatment can reduce a rapid heart rate and high pulmonary artery pressure and can improve the gas exchange indices and outcomes. Surgical embolectomy is also performed in patients with contraindications for or an inadequate response to thrombolysis. Large hospitals having an intensive care unit should preemptively establish diagnostic and therapeutic protocols and rehearse multidisciplinary management for patients with high-risk PE. Coordination with a skilled team comprising intensivists, cardiologists, cardiac surgeons, radiologists, and other specialists is crucial to maximize success.
高危肺栓塞(PE)是一种危及生命的疾病,死亡率和发病率都很高。休克患者的大多数死亡发生在就诊后的最初几个小时内,因此快速诊断和治疗对于挽救患者生命至关重要。大面积PE的主要表现是急性右心室(RV)衰竭和缺氧。RV压力过载主要与机械性肺血管阻塞和潜在的心肺状态之间的相互作用有关。计算机断层扫描血管造影不仅可以清晰显示至少至段级别的肺血栓栓塞,还能显示RV扩大作为RV功能障碍的指标。在这种情况下,床边超声心动图是一种可接受的替代方法。虽然它通常不能提供明确的诊断或排除肺栓塞,但超声心动图可以确认或排除严重的RV压力过载和功能障碍。体外膜肺氧合支持对PE引起的循环衰竭患者可能是一种有效的治疗方法。溶栓治疗一般被接受用于高危PE的不稳定患者;然而,有高出血风险的患者不能充分使用溶栓药物。相反,导管定向治疗是有溶栓禁忌证的高危PE患者的最佳治疗策略,是手术取栓的微创替代方法。它可以使用最小剂量的溶栓药物或不使用溶栓药物进行,并且可以根据肺动脉造影上血栓的范围与包括导管碎栓或取栓在内的各种操作相结合。混合导管定向治疗可以降低快速心率和高肺动脉压,并可以改善气体交换指标和治疗结果。对于有溶栓禁忌证或溶栓反应不佳的患者也会进行手术取栓。拥有重症监护病房的大型医院应预先制定诊断和治疗方案,并对高危PE患者进行多学科管理演练。与由重症医学专家、心脏病专家、心脏外科医生、放射科医生和其他专家组成的专业团队进行协调对于取得最大成功至关重要。