Olivia Newton-John Cancer Research Institute, Heidelberg, VIC, Australia.
School of Cancer Medicine, La Trobe University, Heidelberg, VIC, Australia.
Front Immunol. 2018 Mar 2;9:411. doi: 10.3389/fimmu.2018.00411. eCollection 2018.
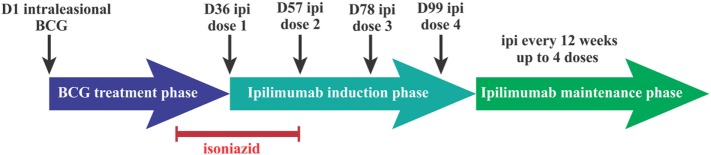
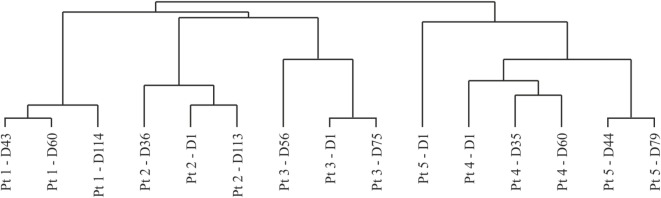
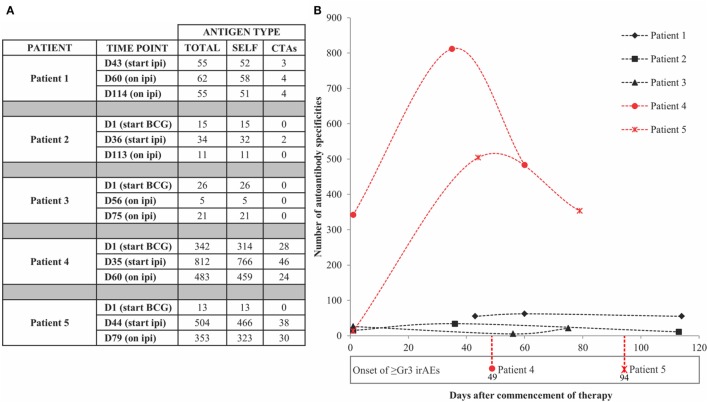
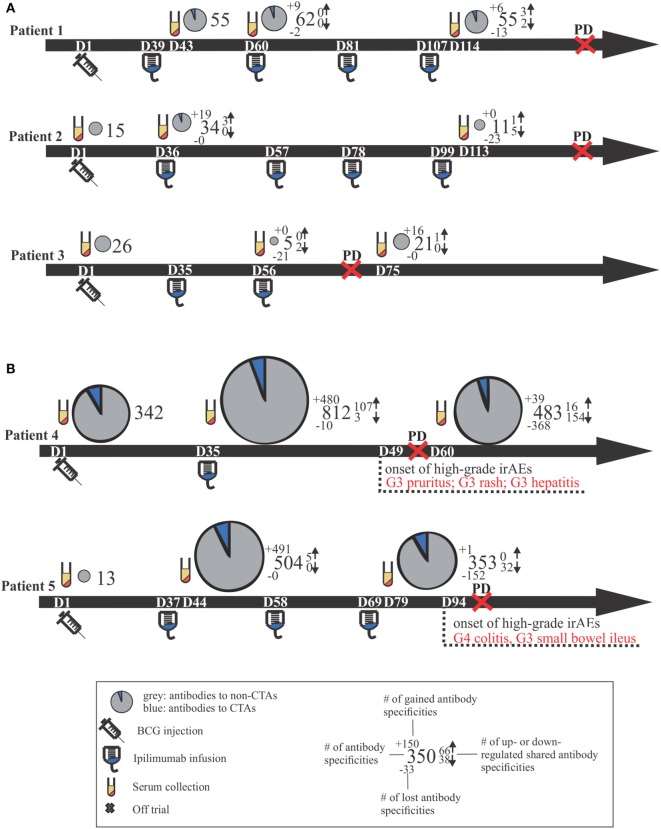
Immune checkpoint inhibitors (ICIs) have revolutionized the treatment of advanced melanoma. The first ICI to demonstrate clinical benefit, ipilimumab, targets cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4); however, the long-term overall survival is just 22%. More than 40 years ago intralesional (IL) (BCG), a living attenuated strain of , was found to induce tumor regression by stimulating cell-mediated immunity following a localized and self-limiting infection. We evaluated these two immune stimulants in combination with melanoma with the aim of developing a more effective immunotherapy and to assess toxicity. In this phase I study, patients with histologically confirmed stage III/IV metastatic melanoma received IL BCG injection followed by up to four cycles of intravenous ipilimumab (anti-CTLA-4) (ClinicalTrials.gov number NCT01838200). The trial was discontinued following treatment of the first five patients as the two patients receiving the escalation dose of BCG developed high-grade immune-related adverse events (irAEs) typical of ipilimumab monotherapy. These irAEs were characterized in both patients by profound increases in the repertoire of autoantibodies directed against both self- and cancer antigens. Interestingly, the induced autoantibodies were detected at time points that preceded the development of symptomatic toxicity. There was no overlap in the antigen specificity between patients and no evidence of clinical responses. Efforts to increase response rates through the use of novel immunotherapeutic combinations may be associated with higher rates of irAEs, thus the imperative to identify biomarkers of toxicity remains strong. While the small patient numbers in this trial do not allow for any conclusive evidence of predictive biomarkers, the observed changes warrant further examination of autoantibody repertoires in larger patient cohorts at risk of developing irAEs during their course of treatment. In summary, dose escalation of IL BCG followed by ipilimumab therapy was not well tolerated in advanced melanoma patients and showed no evidence of clinical benefit. Measuring autoantibody responses may provide early means for identifying patients at risk from developing severe irAEs during cancer immunotherapy.
免疫检查点抑制剂(ICIs)改变了晚期黑色素瘤的治疗格局。首个具有临床获益的ICI,伊匹单抗,作用于细胞毒性 T 淋巴细胞相关抗原-4(CTLA-4);然而,长期的总生存率仅为 22%。40 多年前,研究发现局部、自限性感染后,通过刺激细胞介导的免疫,可诱导肿瘤消退,这使得卡介苗(BCG)发挥作用。BCG 是一种减毒活菌株。我们评估了这两种免疫刺激剂与黑色素瘤联合应用的效果,以期开发更有效的免疫疗法并评估其毒性。在这项 I 期研究中,组织学确诊的 III/IV 期转移性黑色素瘤患者接受局部注射卡介苗(BCG),随后最多接受 4 个周期的静脉注射伊匹单抗(抗 CTLA-4)(ClinicalTrials.gov 编号:NCT01838200)。由于前 5 名患者接受了递增剂量的 BCG 治疗后,2 名患者出现了与伊匹单抗单药治疗相关的高级别免疫相关不良事件(irAEs),该试验停止了。这些 irAEs 的特点是针对自身和癌症抗原的自身抗体谱显著增加。有趣的是,在出现症状性毒性之前的时间点就检测到了诱导的自身抗体。两名患者的抗原特异性没有重叠,也没有临床反应的证据。通过使用新型免疫治疗组合来提高反应率可能会导致更高的 irAE 发生率,因此,识别毒性的生物标志物仍然是当务之急。尽管该试验中患者数量较少,无法提供任何关于预测生物标志物的明确证据,但观察到的变化需要在更大的患者队列中进一步检查自身抗体谱,这些患者在治疗过程中可能会发生 irAE。总的来说,在晚期黑色素瘤患者中,递增剂量的局部 BCG 联合伊匹单抗治疗耐受性不佳,也没有临床获益的证据。测量自身抗体反应可能为识别癌症免疫治疗过程中发生严重 irAE 的风险患者提供早期手段。