Department of Infectious Diseases, Barwon Health, Geelong, Australia.
Department of Medicine and Infectious Diseases, Royal Melbourne Hospital, University of Melbourne, Melbourne, Australia.
PLoS Negl Trop Dis. 2018 Mar 19;12(3):e0006357. doi: 10.1371/journal.pntd.0006357. eCollection 2018 Mar.
Healing times following treatment with antibiotics, and factors that influence healing, have not been reported in Australian patients with Mycobacterium ulcerans.
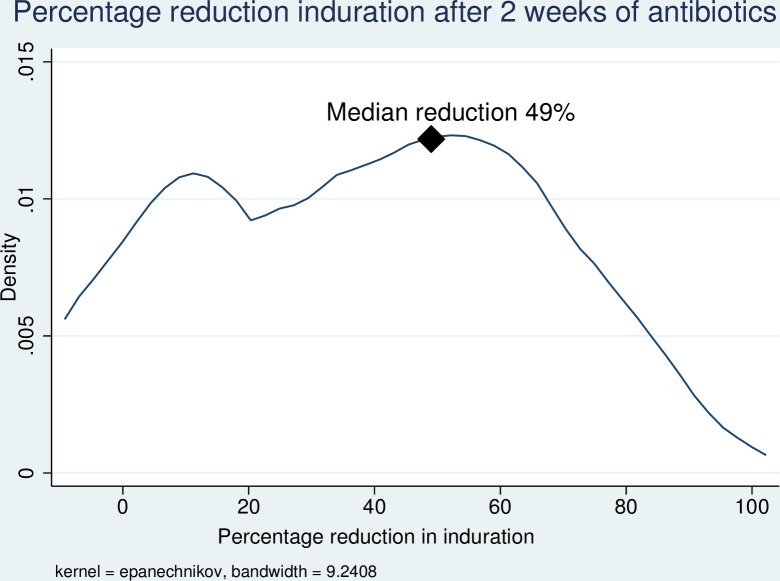
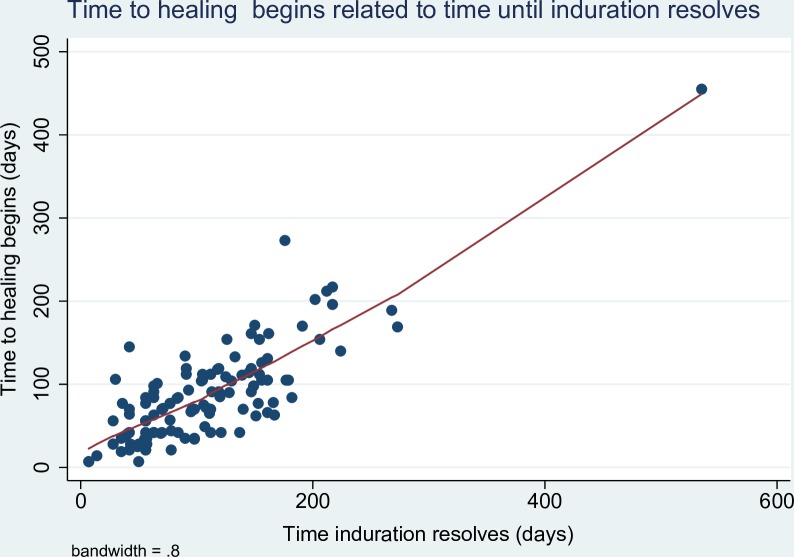
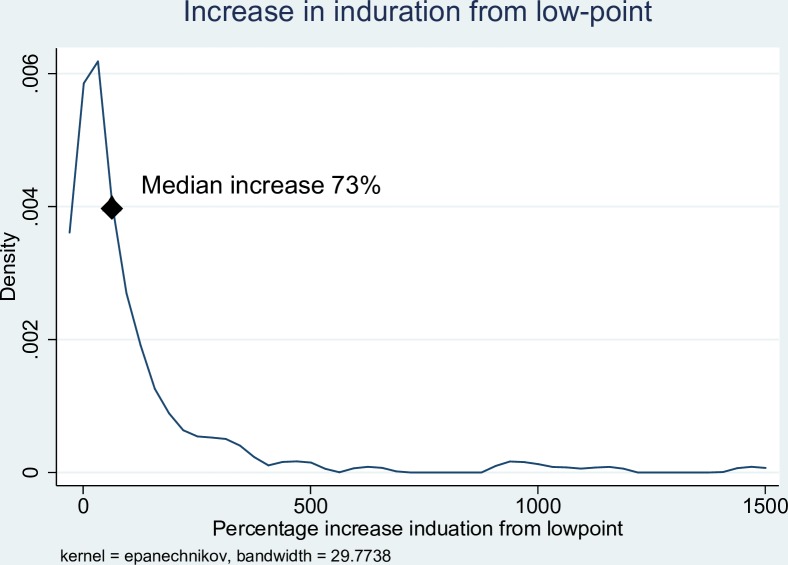
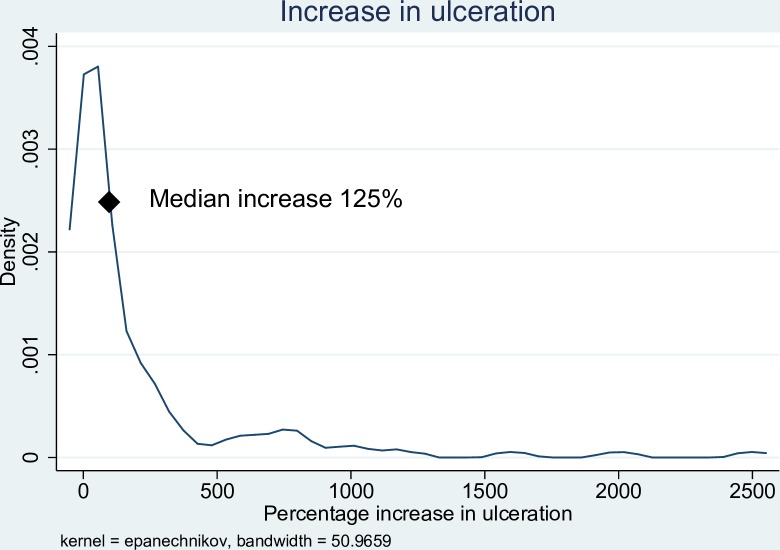
METHODOLOGY/PRINCIPAL FINDINGS: Healing times were determined for all M. ulcerans cases treated by a single physician with antibiotics at Barwon Health, Victoria, from 1/1/13-31/12/16. Lesions were categorised by induration size: category A ≤ 400mm2, Category B 401-1600mm2 and Category C ≥1601mm2. A logistic regression analysis was performed to determine risk factors for prolonged wound healing (>150 days from antibiotic commencement). 163 patients were included; 92 (56.4%) were male and median age was 58 years (IQR 39-73 years). Baseline lesion size [available in 145 (89.0%) patients] was categorised as A in 46 (31.7%), B in 67 (46.2%) and C in 32 (22.1%) patients. Fifty (30.7%) patients had surgery. In those treated with antibiotics alone, 83.0% experienced a reduction in induration size after 2 weeks, then 70.9% experienced an increase in induration size from the lowest point, and 71.7% experienced an increase in ulceration size. A linear relationship existed between the time induration resolved and wound healing began. Median time to heal was 91 days (IQR 70-148 days) for category A lesions; significantly shorter than for category B lesions (128 days, IQR 91-181 days, p = 0.05) and category C lesions (169 days, IQR 159-214 days, p<0.001). Fifty-seven (35.0%) patients experienced a paradoxical reaction. Of those treated with antibiotics alone, lesions experiencing a paradoxical reaction had longer healing times [median time to heal 177 days (IQR 154-224 days) compared to 107 days (IQR 79-153 days), p<0.001]. On multivariable logistic regression, lesion size at baseline (p<0.001) and paradoxical reactions (p<0.001) were independently associated with prolonged healing times. For category A and B lesions, healing time was significantly shorter with antibiotics plus excision and direct closure compared with antibiotics alone [Category A lesions median 55 days (IQR 21-63 days) compared with 91 days (IQR 70-148 days), p<0.001; Category B lesions median 74 days (IQR 21-121 days) compared to 128 days (IQR 97-181 days), p<0.001].
In Australian patients treated with antibiotics M. ulcerans lesions usually initially improve, then clinically deteriorate with increased induration and ulceration, before healing after the inflammation associated with lesions resolves. The time to complete healing of lesions is generally long, and is further prolonged in those with larger initial lesion size or who develop paradoxical reactions. For small lesions (<4cm2), excisional surgery may reduce healing times.
在澳大利亚患有溃疡分枝杆菌的患者中,尚未报道抗生素治疗后的愈合时间以及影响愈合的因素。
方法/主要发现:对 2013 年 1 月 1 日至 2016 年 12 月 31 日期间在维多利亚州巴旺健康中心接受单一医生抗生素治疗的所有溃疡分枝杆菌病例的愈合时间进行了确定。根据硬结大小对病变进行分类:A 类≤400mm2,B 类 401-1600mm2,C 类≥1601mm2。进行逻辑回归分析以确定延长伤口愈合(抗生素开始后>150 天)的风险因素。纳入 163 例患者;92 例(56.4%)为男性,中位年龄为 58 岁(IQR 39-73 岁)。基线病变大小[145 例(89.0%)患者中可获得]在 46 例(31.7%)中为 A 类,在 67 例(46.2%)中为 B 类,在 32 例(22.1%)中为 C 类。50 例(30.7%)患者进行了手术。在单独使用抗生素治疗的患者中,83.0%的患者在第 2 周后硬结缩小,然后 70.9%的患者硬结从最低点开始增加,71.7%的患者溃疡增大。硬结消退与开始愈合之间存在线性关系。A 类病变的中位愈合时间为 91 天(IQR 70-148 天);显著短于 B 类病变(128 天,IQR 91-181 天,p = 0.05)和 C 类病变(169 天,IQR 159-214 天,p<0.001)。57 例(35.0%)患者出现反常反应。在单独使用抗生素治疗的患者中,出现反常反应的病变愈合时间更长[中位愈合时间为 177 天(IQR 154-224 天),而 107 天(IQR 79-153 天),p<0.001]。在多变量逻辑回归中,基线病变大小(p<0.001)和反常反应(p<0.001)与延长愈合时间独立相关。对于 A 类和 B 类病变,抗生素加切除和直接闭合的愈合时间明显短于单独使用抗生素[A 类病变中位 55 天(IQR 21-63 天),91 天(IQR 70-148 天),p<0.001;B 类病变中位 74 天(IQR 21-121 天)与 128 天(IQR 97-181 天)相比,p<0.001]。
在接受抗生素治疗的澳大利亚患者中,分枝杆菌溃疡病变通常最初会改善,然后在与病变相关的炎症消退之前,临床病情恶化,硬结和溃疡增大,然后再愈合。病变完全愈合的时间通常较长,在初始病变较大或出现反常反应的患者中进一步延长。对于小病变(<4cm2),切除手术可能会缩短愈合时间。