School of Traditional Chinese Medicine, Southern Medical University, Guangzhou, Guangdong, China (mainland).
Department of Otolaryngology, Head and Neck Surgery, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, China (mainland).
Med Sci Monit. 2018 Apr 26;24:2562-2568. doi: 10.12659/MSM.906625.
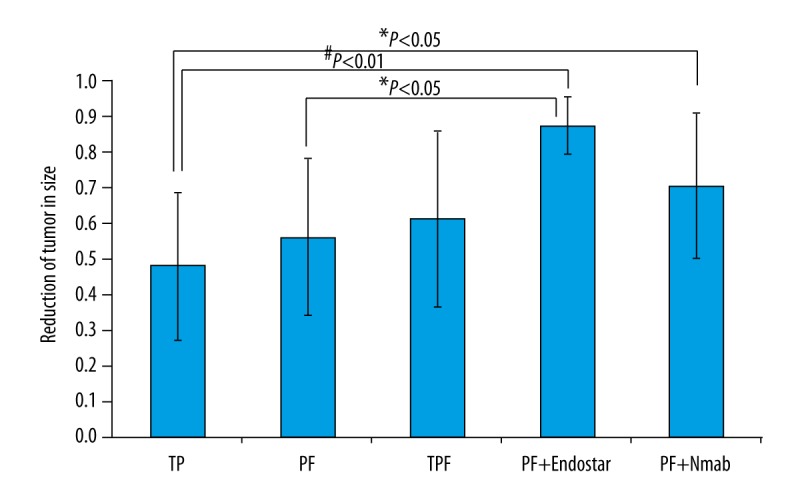
BACKGROUND Combined chemotherapy and radiation therapy are used to treat nasopharyngeal carcinoma (NPC). Previous studies have shown that induction chemotherapy, given before radiotherapy, is beneficial in patients with local lymph node metastases. The aim of this study was to evaluate regional lymph node size in patients with NPC and the efficacy of five induction chemotherapy regimens given before radiotherapy. MATERIAL AND METHODS Between December 2007 and June 2011, 190 patients were included in this study, who had regionally advanced NPC (Stages II-IV). Five induction chemotherapy regimens were given prior to radiation: 98 patients (51.6%) received the TPF regimen (docetaxel, cisplatin, and fluorouracil); 56 patients (29.5%) received PF regimen (cisplatin and fluorouracil); 26 patients (13.7%) received the TP regimen (cisplatin and docetaxel); seven patients (3.7%) received combined nimotuzumab with TPF; three patients (1.6%) received a combination of the novel modified recombinant human endostatin (Endostar) with PF. The length and width of the regional lymph nodes were measured using neck B-mode (high-resolution grey scale) ultrasonography before chemotherapy and on the second day following completion of chemotherapy. Gastrointestinal tract and bone marrow suppression were also monitored during and after chemotherapy. RESULTS The TPF chemotherapy induction regimen resulted in an improved early response of lymph node size reduction, compared with the PF and TP chemotherapy induction regimens. The combined use of nimotuzumab with the TPF regimen improved efficacy by 15%. The combined use of Endostar improved the efficacy of the PF regimen by 56% (P<0.05). CONCLUSIONS In a retrospective study in patients with NPC, different induction chemotherapy regimens had different effects on lymph node size before radiation therapy.
联合化疗和放疗用于治疗鼻咽癌(NPC)。先前的研究表明,在放疗前进行诱导化疗对有局部淋巴结转移的患者有益。本研究旨在评估 NPC 患者的区域淋巴结大小以及放疗前给予的五种诱导化疗方案的疗效。
2007 年 12 月至 2011 年 6 月,共纳入 190 例局部晚期 NPC(II-IV 期)患者。在放疗前给予五种诱导化疗方案:98 例(51.6%)患者接受 TPF 方案(多西紫杉醇、顺铂和氟尿嘧啶);56 例(29.5%)患者接受 PF 方案(顺铂和氟尿嘧啶);26 例(13.7%)患者接受 TP 方案(顺铂和多西紫杉醇);7 例(3.7%)患者接受 TPF 联合尼妥珠单抗治疗;3 例(1.6%)患者接受新型重组人血管内皮抑制素(恩度)联合 PF 方案治疗。在化疗前和化疗结束后第二天,使用颈部 B 型(高分辨率灰阶)超声测量区域淋巴结的长度和宽度。在化疗期间和之后还监测了胃肠道和骨髓抑制情况。
TPF 化疗诱导方案与 PF 和 TP 化疗诱导方案相比,可改善淋巴结缩小的早期反应。尼妥珠单抗联合 TPF 方案可提高疗效 15%。恩度联合 PF 方案可提高疗效 56%(P<0.05)。
在 NPC 患者的回顾性研究中,不同的诱导化疗方案对放疗前的淋巴结大小有不同的影响。