Centre for Healthcare Resilience and Implementation Science, Australian Institute of Health Innovation, Macquarie University, Level 6, 75 Talavera Road, North Ryde, NSW, 2109, Australia.
BMC Med. 2018 Apr 30;16(1):63. doi: 10.1186/s12916-018-1057-z.
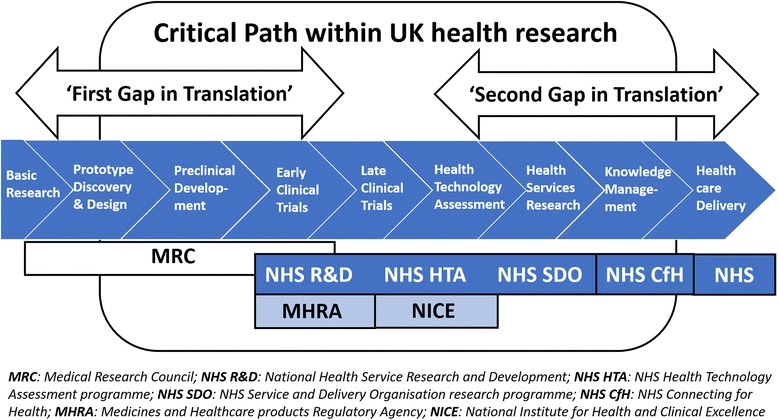
Implementation science has a core aim - to get evidence into practice. Early in the evidence-based medicine movement, this task was construed in linear terms, wherein the knowledge pipeline moved from evidence created in the laboratory through to clinical trials and, finally, via new tests, drugs, equipment, or procedures, into clinical practice. We now know that this straight-line thinking was naïve at best, and little more than an idealization, with multiple fractures appearing in the pipeline.
The knowledge pipeline derives from a mechanistic and linear approach to science, which, while delivering huge advances in medicine over the last two centuries, is limited in its application to complex social systems such as healthcare. Instead, complexity science, a theoretical approach to understanding interconnections among agents and how they give rise to emergent, dynamic, systems-level behaviors, represents an increasingly useful conceptual framework for change. Herein, we discuss what implementation science can learn from complexity science, and tease out some of the properties of healthcare systems that enable or constrain the goals we have for better, more effective, more evidence-based care. Two Australian examples, one largely top-down, predicated on applying new standards across the country, and the other largely bottom-up, adopting medical emergency teams in over 200 hospitals, provide empirical support for a complexity-informed approach to implementation. The key lessons are that change can be stimulated in many ways, but a triggering mechanism is needed, such as legislation or widespread stakeholder agreement; that feedback loops are crucial to continue change momentum; that extended sweeps of time are involved, typically much longer than believed at the outset; and that taking a systems-informed, complexity approach, having regard for existing networks and socio-technical characteristics, is beneficial.
Construing healthcare as a complex adaptive system implies that getting evidence into routine practice through a step-by-step model is not feasible. Complexity science forces us to consider the dynamic properties of systems and the varying characteristics that are deeply enmeshed in social practices, whilst indicating that multiple forces, variables, and influences must be factored into any change process, and that unpredictability and uncertainty are normal properties of multi-part, intricate systems.
实施科学的核心目标是将证据转化为实践。在循证医学运动的早期,这项任务被构造成线性的,其中知识管道从实验室中创建的证据通过临床试验,最后通过新的测试、药物、设备或程序,进入临床实践。我们现在知道,这种直线思维充其量是幼稚的,只不过是一种理想化,在管道中出现了多个裂缝。
知识管道源自于对科学的机械线性方法,虽然在过去两个世纪中为医学带来了巨大的进步,但在应用于复杂的医疗保健等社会系统时,其应用受到限制。相反,复杂性科学是一种理解代理之间相互关系以及它们如何产生涌现、动态、系统级行为的理论方法,为变革提供了一个越来越有用的概念框架。在这里,我们讨论了实施科学可以从复杂性科学中学到什么,并梳理出一些医疗保健系统的特性,这些特性可以促进或限制我们实现更好、更有效、更基于证据的护理的目标。澳大利亚的两个例子,一个主要是自上而下的,基于在全国范围内应用新标准,另一个主要是自下而上的,在 200 多家医院采用医疗急救小组,为实施基于复杂性的方法提供了经验支持。关键教训是,改变可以通过多种方式来刺激,但需要一个触发机制,如立法或广泛的利益相关者共识;反馈循环对于继续改变动力至关重要;需要涉及扩展的时间范围,通常比一开始认为的要长得多;以及采取系统的、复杂性的方法,考虑到现有的网络和社会技术特征,是有益的。
将医疗保健视为一个复杂的自适应系统意味着,通过逐步的模型将证据应用于常规实践是不可行的。复杂性科学迫使我们考虑系统的动态特性和深深嵌入社会实践中的各种特征,同时表明,任何变革过程都必须考虑到多种力量、变量和影响,不可预测性和不确定性是多部分复杂系统的正常特性。