Harvin John A, Podbielski Jeanette, Vincent Laura E, Fox Erin E, Moore Laura J, Cotton Bryan A, Wade Charles E, Holcomb John B
Department of Surgery, McGovern Medical School, The University of Texas Health Science Center at Houston, Houston, Texas, USA.
The Center for Translational Injury Research, McGovern Medical School, The University of Texas Health Science Center at Houston, Houston, Texas, USA.
Trauma Surg Acute Care Open. 2017 Apr 13;2(1):e000083. doi: 10.1136/tsaco-2017-000083. eCollection 2017.
Damage control laparotomy (DCL) is an abbreviated operation intended to prevent the development of hypothermia, acidosis, and coagulopathy in seriously injured patients. The indications for DCL have since been broadened with no high-quality data to guide treatment. For patients with an indication for DCL, we aim to determine the effect of definitive laparotomy on patient morbidity.
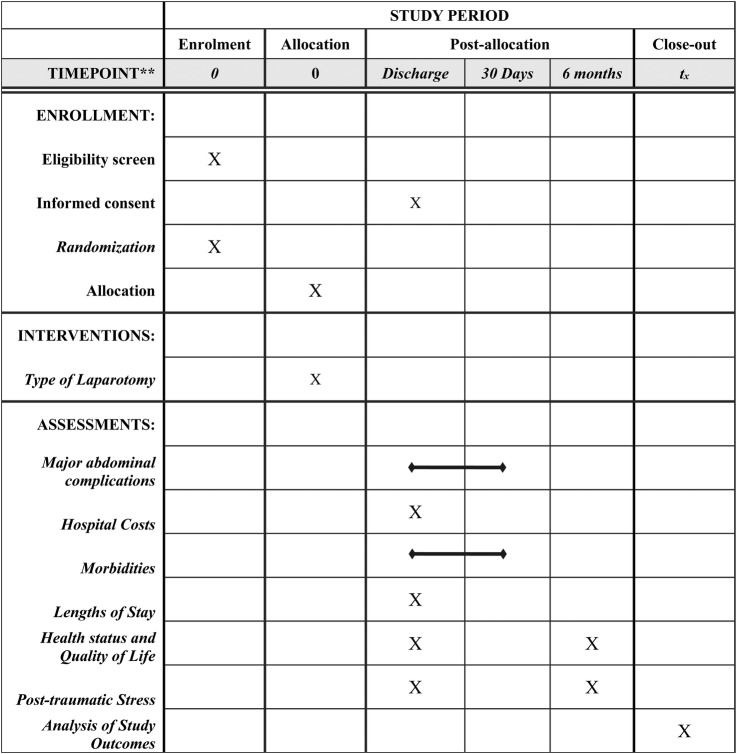
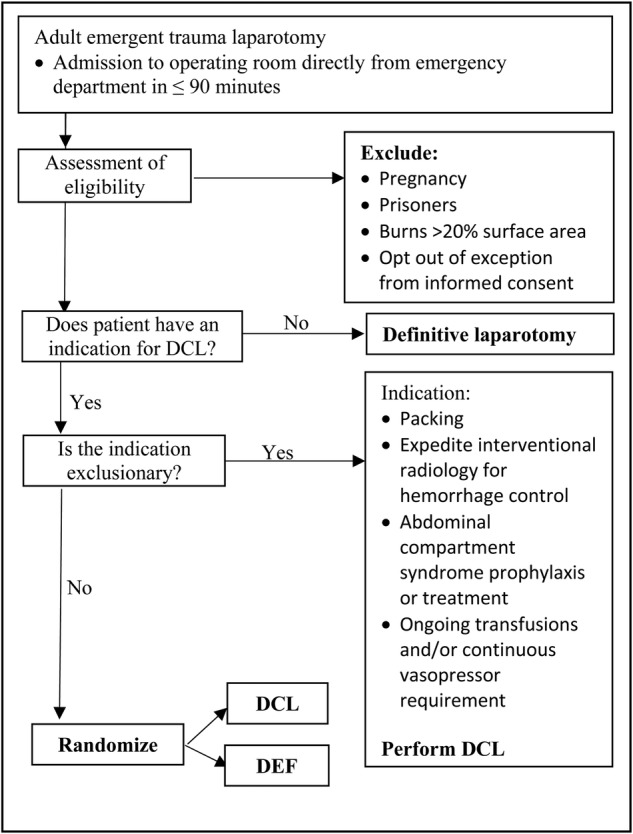
This is a pragmatic, parallel-group, randomized controlled pilot trial. Emergent laparotomy is defined as admission directly to the operating room from the emergency department within 90 min of arrival. DCL indications excluded from the study include packing of the liver or retroperitoneum, abdominal compartment syndrome prophylaxis, to expedite interventional radiology for hemorrhage control, and the need for ongoing transfusions and/or continuous vasopressor support. When a surgeon determines a DCL is indicated, the patient will be screened for inclusion and exclusion criteria. Patients with any indication for DCL that is not excluded are eligible for randomization. Patients will be randomized intraoperatively to DCL (control) or definitive fascial closure of the laparotomy (intervention). The primary outcome will be major abdominal complication or death within 30 days. Major abdominal complication is a composite outcome including fascial dehiscence, organ/space surgical site infection, enteric suture line failure, and unplanned reopening of the abdomen. Outcomes will be compared using both frequentist and Bayesian statistics.
In patients with an indication for DCL, this trial will determine the effect of definitive laparotomy on major abdominal complications and death and will inform clinicians on the risks and benefits of this procedure. Regardless of the study outcome, the results will improve the quality of care provided to injured patients.
NCT02706041.
损伤控制剖腹术(DCL)是一种简化手术,旨在防止重伤患者发生体温过低、酸中毒和凝血功能障碍。此后,DCL的适应证有所扩大,但缺乏高质量数据来指导治疗。对于有DCL适应证的患者,我们旨在确定确定性剖腹术对患者发病率的影响。
这是一项务实的、平行组、随机对照试验。急诊剖腹术定义为在到达后90分钟内从急诊科直接进入手术室。本研究排除的DCL适应证包括肝脏或腹膜后填塞、预防腹腔间隔室综合征、加快介入放射学控制出血以及持续输血和/或持续血管活性药物支持的需要。当外科医生确定需要进行DCL时,将对患者进行纳入和排除标准筛查。任何未被排除的有DCL适应证的患者都有资格随机分组。患者将在术中随机分为DCL组(对照组)或确定性剖腹术筋膜关闭组(干预组)。主要结局将是30天内发生的严重腹部并发症或死亡。严重腹部并发症是一个综合结局,包括筋膜裂开、器官/腔隙手术部位感染、肠吻合口漏和计划外的腹部再次开放。将使用频率统计和贝叶斯统计对结局进行比较。
对于有DCL适应证的患者,本试验将确定确定性剖腹术对严重腹部并发症和死亡的影响,并将告知临床医生该手术的风险和益处。无论研究结果如何,这些结果都将提高为受伤患者提供的护理质量。
NCT02706041。