Baylor Heart and Vascular Institute, Baylor Scott & White Research Institute, Dallas, TX.
Department of Internal Medicine, Texas A&M University College of Medicine Health Science Center, Dallas, TX.
J Am Heart Assoc. 2018 May 17;7(11):e008377. doi: 10.1161/JAHA.117.008377.
Vasoplegia is associated with adverse outcomes following cardiac surgery; however, its impact following left ventricular assist device implantation is largely unexplored.
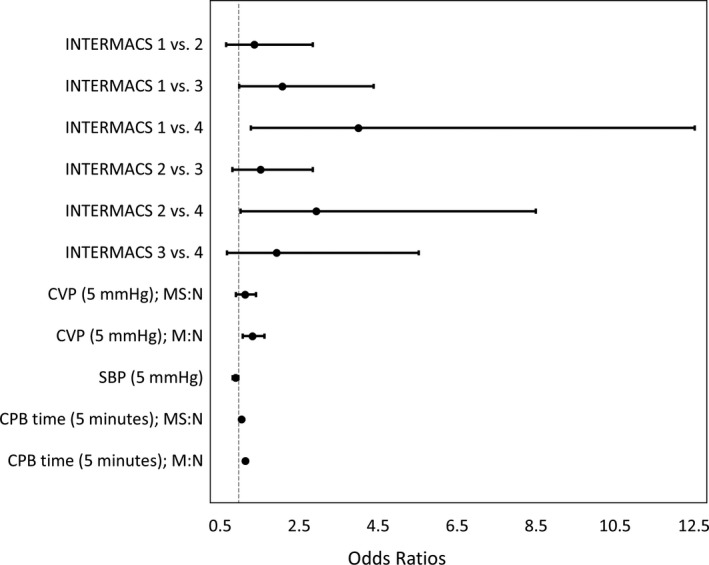
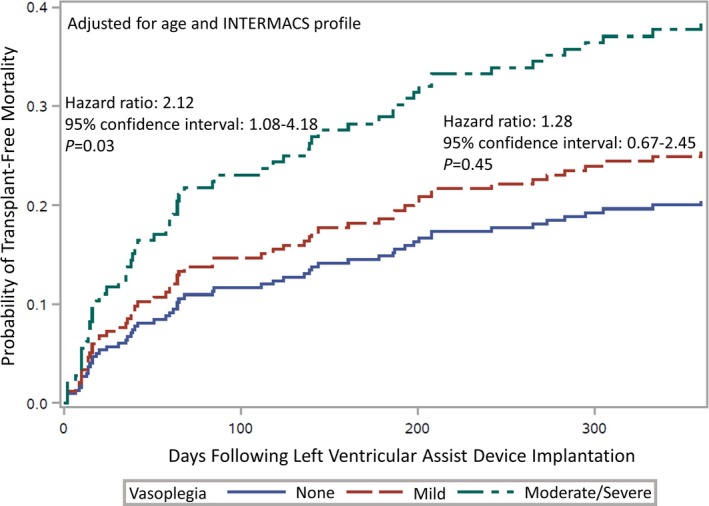
In 252 consecutive patients receiving a left ventricular assist device, vasoplegia was defined as the occurrence of normal cardiac function and index but with the need for intravenous vasopressors within 48 hours following surgery for >24 hours to maintain a mean arterial pressure >70 mm Hg. We further categorized vasoplegia as ; , requiring 1 vasopressor (vasopressin, norepinephrine, or high-dose epinephrine [>5 μg/min]); or , requiring ≥2 vasopressors. Predictors of vasoplegia severity were determined using a cumulative logit (ordinal logistic regression) model, and 1-year mortality was evaluated using competing-risks survival analysis. In total, 67 (26.6%) patients developed mild vasoplegia and 57 (22.6%) developed moderate to severe vasoplegia. The multivariable model for vasoplegia severity utilized preoperative Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) profile, central venous pressure, systolic blood pressure, and intraoperative cardiopulmonary bypass time, which yielded an area under the curve of 0.76. Although no significant differences were noted in stroke or pump thrombosis rates (=0.87 and =0.66, respectively), respiratory failure and major bleeding increased with vasoplegia severity (<0.01). Those with moderate to severe vasoplegia had a significantly higher risk of mortality than those without vasoplegia (adjusted hazard ratio: 2.12; 95% confidence interval, 1.08-4.18; =0.03).
Vasoplegia is predictive of unfavorable outcomes, including mortality. Risk factors for future research include preoperative INTERMACS profile, central venous pressure, systolic blood pressure, and intraoperative cardiopulmonary bypass time.
心脏手术后发生血管麻痹与不良结局相关;然而,左心室辅助装置植入术后发生血管麻痹的情况在很大程度上尚未被探索。
在 252 例连续接受左心室辅助装置治疗的患者中,血管麻痹定义为手术 48 小时内出现正常心脏功能和指数,但需要静脉血管加压素治疗>24 小时,以维持平均动脉压>70mmHg。我们进一步将血管麻痹分为轻度,需要 1 种血管加压剂(血管加压素、去甲肾上腺素或高剂量肾上腺素[>5μg/min]);或中重度,需要≥2 种血管加压剂。使用累积对数(有序逻辑回归)模型确定血管麻痹严重程度的预测因素,并使用竞争风险生存分析评估 1 年死亡率。共有 67 例(26.6%)患者发生轻度血管麻痹,57 例(22.6%)患者发生中重度血管麻痹。血管麻痹严重程度的多变量模型使用术前机械循环辅助机构间注册(INTERMACS)评分、中心静脉压、收缩压和术中体外循环时间,其曲线下面积为 0.76。尽管在卒中或泵血栓形成率方面无显著差异(=0.87 和=0.66),但随着血管麻痹严重程度的增加,呼吸衰竭和大出血的发生率也增加(<0.01)。与无血管麻痹患者相比,中重度血管麻痹患者的死亡率显著更高(调整后的危险比:2.12;95%置信区间,1.08-4.18;=0.03)。
血管麻痹是不良结局的预测因素,包括死亡率。未来研究的风险因素包括术前 INTERMACS 评分、中心静脉压、收缩压和术中体外循环时间。