Alshahrani Abdulwahab A, Hwang Shin, Song Gi-Won, Moon Deok-Bog, Jung Dong-Hwan, Ahn Chul-Soo, Kim Ki-Hun, Ha Tae-Yong, Park Gil-Chun, Ha Su-Min, Park Yo-Han, Lee Sung-Gyu
Division of Hepatobiliary Surgery and Liver Transplantation, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Multi Organ Transplant Center, King Fahad Specialist University Hospital, Dammam, Saudi Arabia.
Ann Hepatobiliary Pancreat Surg. 2018 May;22(2):136-143. doi: 10.14701/ahbps.2018.22.2.136. Epub 2018 May 30.
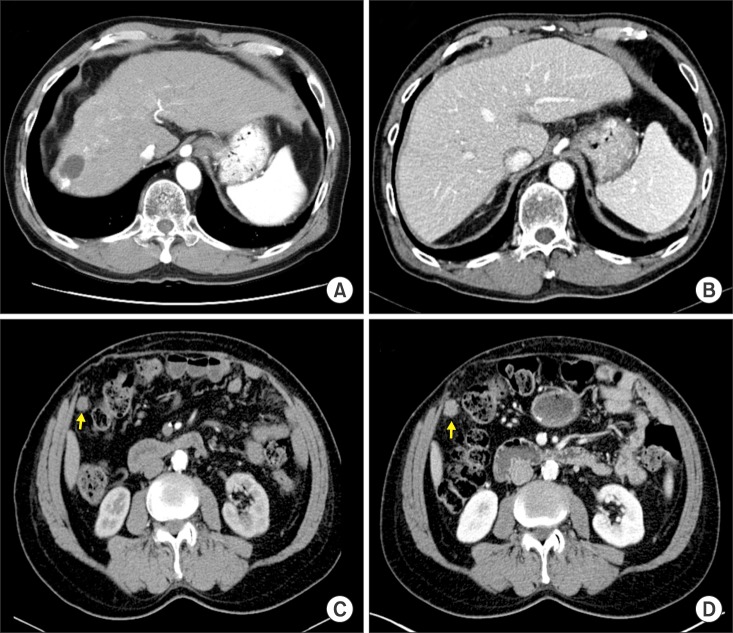
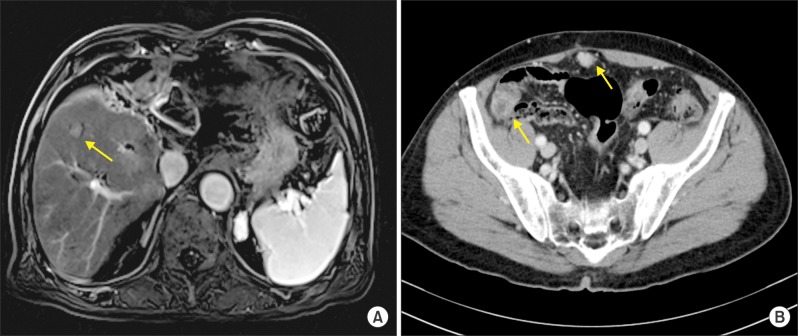
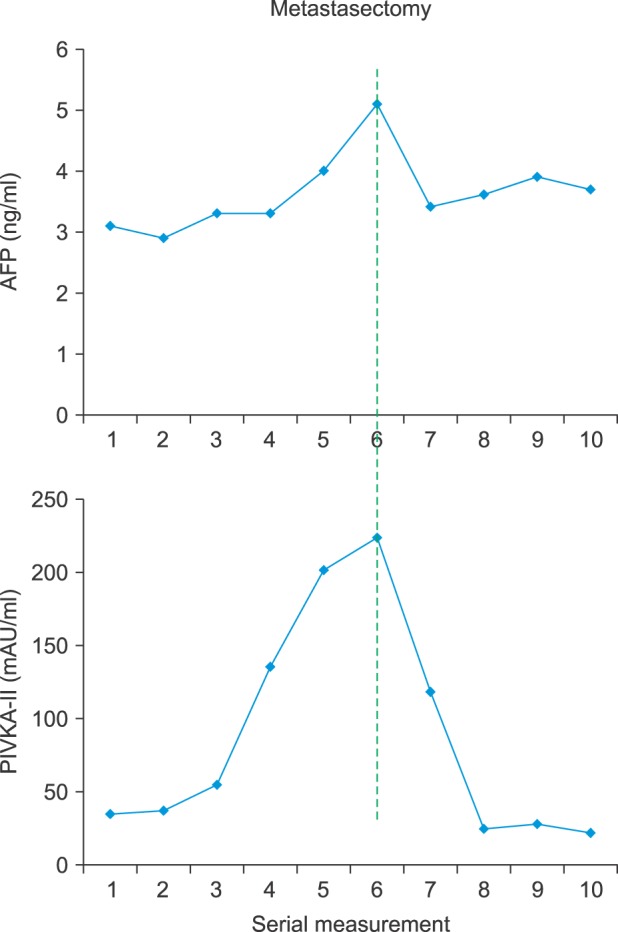
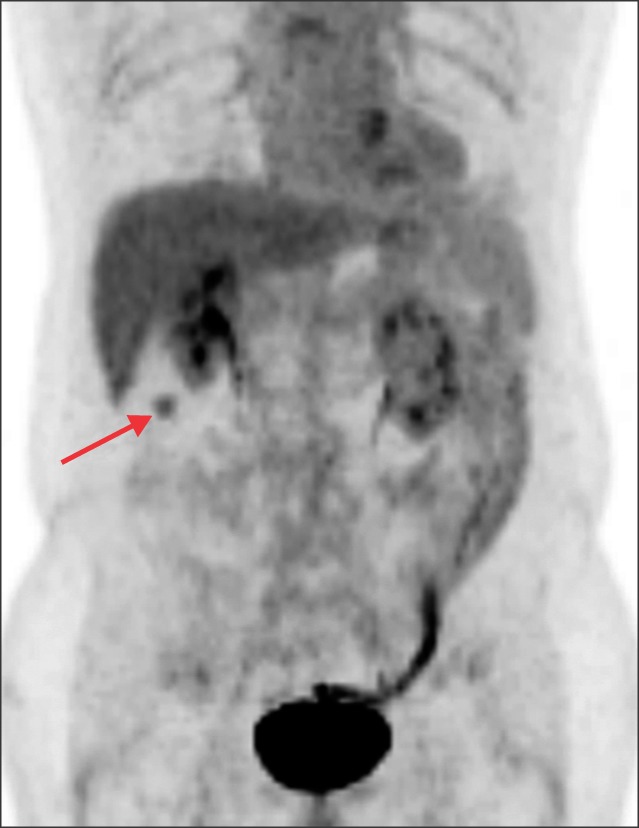
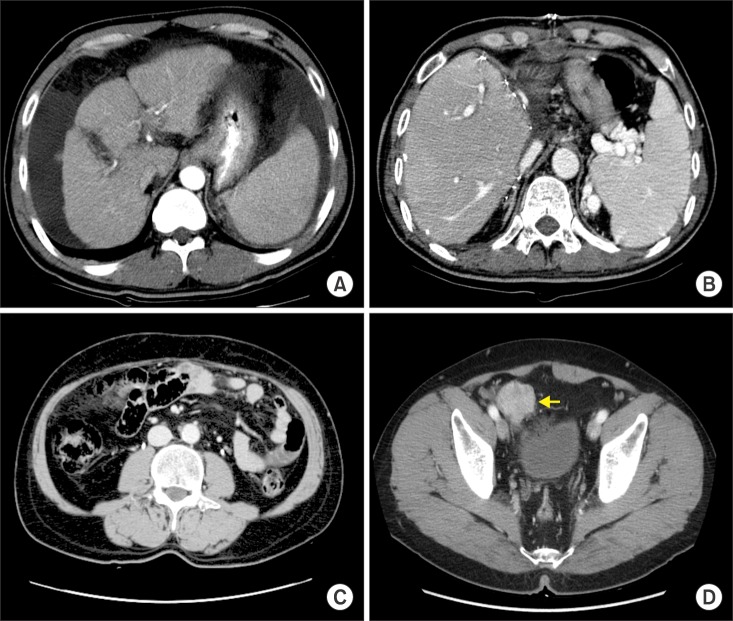
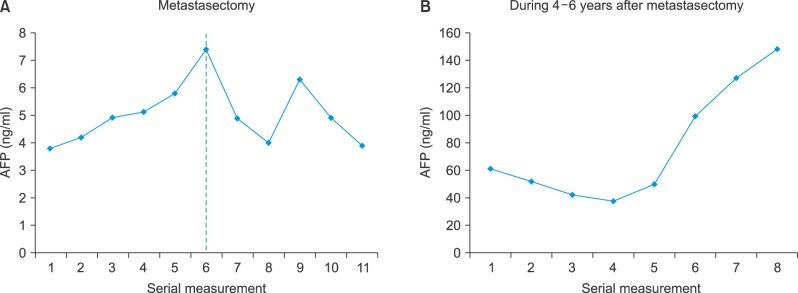
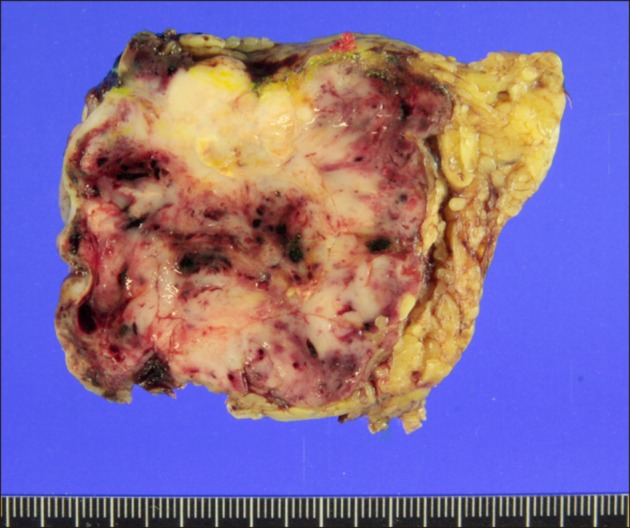
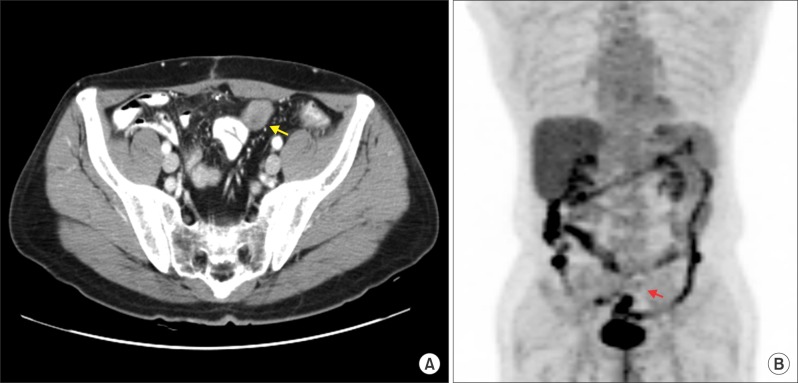
Recurrence of hepatocellular carcinoma (HCC) 10 years after liver transplantation (LT) is very rare. Here, we present two cases of peritoneal metastasis of HCC that occurred 10 and 12 years after LT. A 77-year-old male who had undergone deceased-donor LT 10 years earlier showed slow progressive elevation of tumor marker levels over 6 months. Close observation with frequent imaging studies and monthly tumor marker analyses revealed a solitary peritoneal seeding mass. Imaging studies revealed that the mass was highly likely to be metastatic HCC. After excision of the mass, all tumor markers returned to the normal range. Over past 10 months, the patient has received everolimus monotherapy and half-dose sorafenib, and has shown no evidence of HCC recurrence. In the second case, marginally elevated tumor marker levels were detected in a 65-year-old male who had undergone living-donor LT 12 years earlier. After observation for 3 months, follow-up studies revealed a peritoneal seeding mass. Thorough imaging studies revealed that the mass was highly likely to be metastatic HCC. Two mass lesions were excised, and the patient was administered low-dose calcineruin inhibitor, sirolimus, and full-dose sorafenib. Subsequently, the tumor marker levels increased again and growth of new peritoneal seeding nodules was observed; therefore, sorafenib was stopped after 2 years of administration. During 6 years since HCC recurrence diagnosis, the patient has experienced slowly growing tumors, but has been doing well. For very late peritoneal metastasis of HCC, the therapeutic modalities include surgical resection if possible, everolimus monotherapy, and long-term use of sorafenib.
肝移植(LT)10年后肝细胞癌(HCC)复发极为罕见。在此,我们报告两例LT术后10年和12年发生的HCC腹膜转移病例。一名77岁男性,10年前接受了尸体供肝LT,在6个月内肿瘤标志物水平缓慢进行性升高。通过频繁的影像学检查和每月的肿瘤标志物分析进行密切观察,发现了一个孤立的腹膜种植性肿块。影像学检查显示该肿块极有可能是转移性HCC。切除肿块后,所有肿瘤标志物均恢复至正常范围。在过去10个月里,该患者接受了依维莫司单药治疗和半量索拉非尼治疗,未出现HCC复发迹象。在第二例中,一名65岁男性,12年前接受了活体供肝LT,检测到肿瘤标志物水平略有升高。观察3个月后,后续研究发现了一个腹膜种植性肿块。全面的影像学检查显示该肿块极有可能是转移性HCC。切除了两个肿块病灶,并给予患者低剂量钙调神经磷酸酶抑制剂、西罗莫司和全量索拉非尼治疗。随后,肿瘤标志物水平再次升高,并观察到新的腹膜种植结节生长;因此,索拉非尼在给药2年后停用。自HCC复发诊断以来的6年里,该患者肿瘤生长缓慢,但情况良好。对于HCC非常晚期的腹膜转移,治疗方式包括尽可能进行手术切除、依维莫司单药治疗以及长期使用索拉非尼。