Metzger Anja K, Segal Nicolas, Olson Dai Wai, Figueroa Stephen A, Sadaka Farid G, Krause Catherine A, Homuth James R, Burkhart Nathaniel T, Neumann Robert T, Lurie Keith G, Convertino Victor A
University of Minnesota, Minneapolis, MN, USA.
ZOLL Minneapolis, St. Paul, MN, USA.
J Med Case Rep. 2018 Jun 26;12(1):178. doi: 10.1186/s13256-018-1720-1.
Reducing intrathoracic pressure in the setting of compromised cerebral perfusion due to acute brain injury has been associated with reduced intracranial pressure and enhanced cerebral perfusion pressure and blood flow in animals. Noninvasive active intrathoracic pressure regulation lowers intrathoracic pressure, increases preload, reduces the volume of venous blood and cerebral spinal fluid in the skull, and enhances cerebral blood flow. We examined the feasibility of active intrathoracic pressure regulation therapy in patients with brain injury. We hypothesized that active intrathoracic pressure regulation therapy would be associated with lowered intracranial pressure and increased cerebral perfusion pressure in these patients.
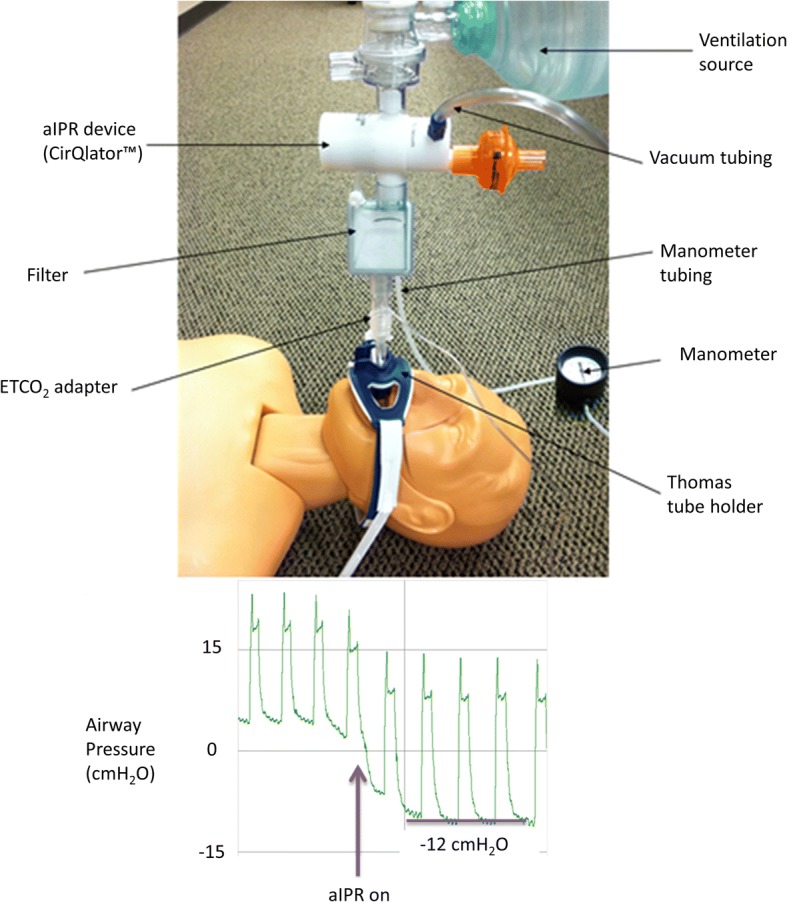
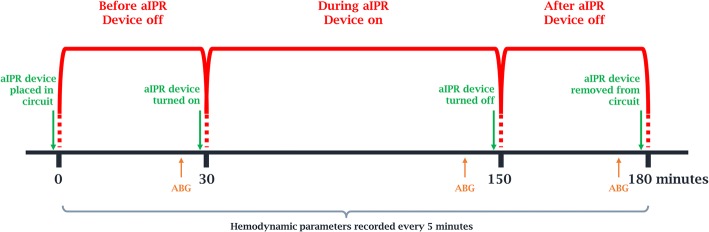
At three institutions, active intrathoracic pressure regulation therapy (CirQlator™, ZOLL) was utilized for 2 consecutive hours in five mechanically ventilated patients with brain injury. A 30-minute interval was used to collect baseline data and determine persistence of effects after device use. End-tidal carbon dioxide was controlled by respiratory rate changes during device use. The intracranial pressure, mean arterial pressure, and cerebral perfusion pressure were recorded at 5-minute intervals throughout all three periods of the protocol. Results for each interval are reported as mean and standard deviation.
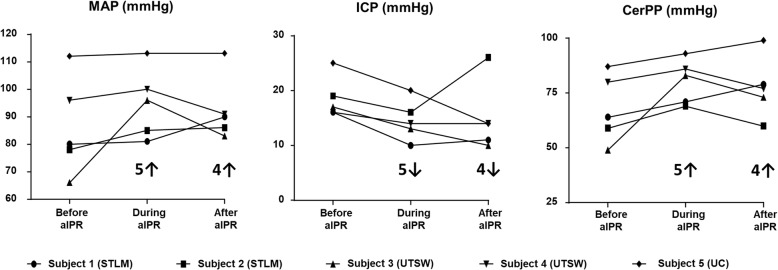
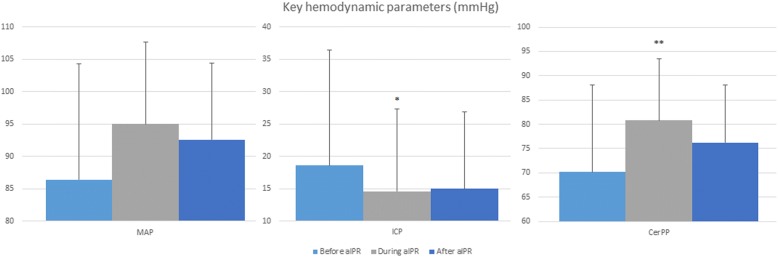
Intracranial pressure was decreased in all five patients by an average of 21% during (15 ± 4 mmHg) compared to before active intrathoracic pressure regulation (19 ± 4) (p = 0.005). This effect on intracranial pressure (15 ± 6) was still present in four of the five patients 30 minutes after therapy was discontinued (p = 0.89). As a result, cerebral perfusion pressure was 16% higher during (81 ± 10) compared to before active intrathoracic pressure regulation (70 ± 14) (p = 0.04) and this effect remained present 30 minutes after therapy was discontinued. No adverse events were reported.
These data support the notion that active intrathoracic pressure regulation, in this limited evaluation, can successfully augment cerebral perfusion by lowering intracranial pressure and increasing mean arterial pressure in patients with mild brain injury. The measured effects were immediate on administration of the therapy and persisted to some degree after the therapy was terminated.
在急性脑损伤导致脑灌注受损的情况下,降低胸内压与动物颅内压降低、脑灌注压和血流量增加有关。无创主动胸内压调节可降低胸内压,增加前负荷,减少颅骨内静脉血和脑脊液的体积,并增加脑血流量。我们研究了主动胸内压调节治疗在脑损伤患者中的可行性。我们假设主动胸内压调节治疗与这些患者颅内压降低和脑灌注压升高有关。
在三个机构中,对五名机械通气的脑损伤患者连续使用主动胸内压调节治疗(CirQlator™,ZOLL)2小时。使用30分钟的间隔来收集基线数据并确定设备使用后的效果持续性。在设备使用期间,通过呼吸频率变化来控制呼气末二氧化碳。在方案的所有三个阶段中,每隔5分钟记录颅内压、平均动脉压和脑灌注压。每个间隔的结果报告为平均值和标准差。
与主动胸内压调节前(19±4)相比,所有五名患者在治疗期间(15±4mmHg)的颅内压平均降低了21%(p = 0.005)。在治疗停止30分钟后,五名患者中有四名患者的颅内压(15±6)仍保持这种效果(p = 0.89)。结果,与主动胸内压调节前(70±14)相比,治疗期间(81±10)的脑灌注压高出16%(p = 0.04),并且在治疗停止30分钟后这种效果仍然存在。未报告不良事件。
这些数据支持这样的观点,即在这项有限的评估中,主动胸内压调节可以通过降低轻度脑损伤患者的颅内压和增加平均动脉压来成功增加脑灌注。所测量的效果在治疗给药后立即出现,并在治疗终止后在一定程度上持续存在。