Department of Critical Care Medicine, Universitair Ziekenhuis Brussel, Vrije Universiteit Brussel, Brussels, Belgium.
Department of Biostatistics, Vrije Universiteit Brussel, Brussels, Belgium.
PLoS One. 2018 Aug 7;13(8):e0200495. doi: 10.1371/journal.pone.0200495. eCollection 2018.
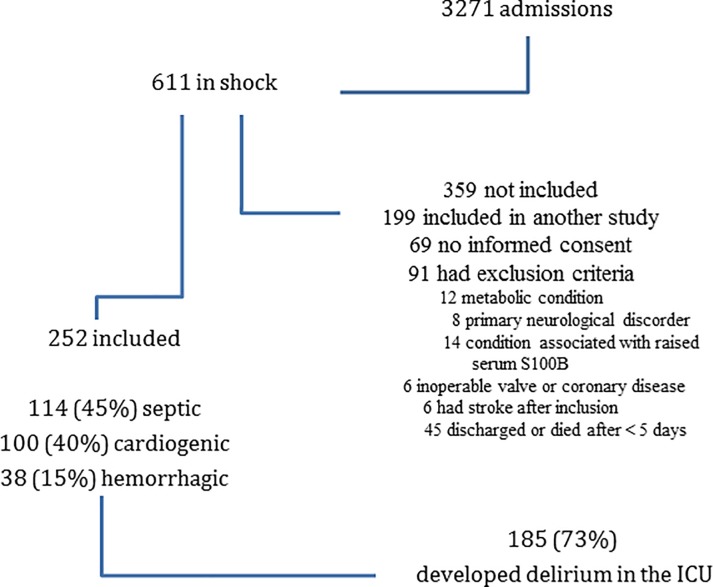
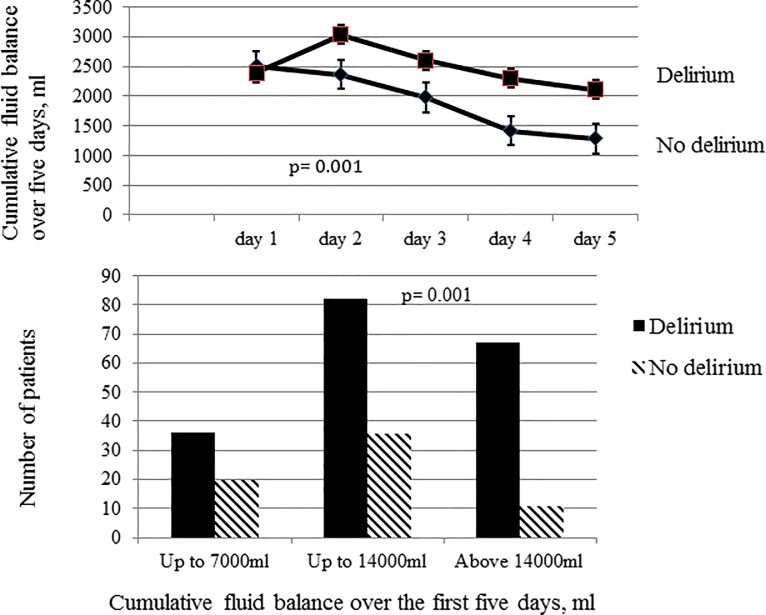
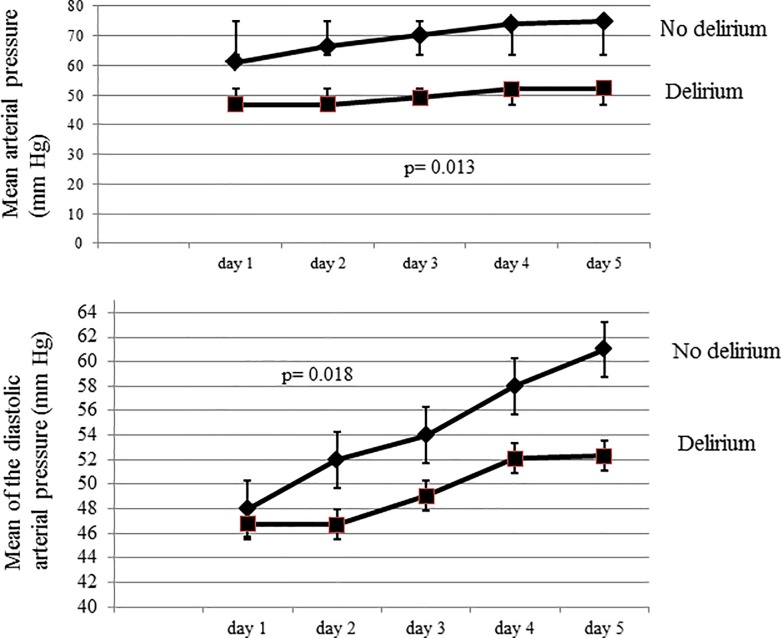
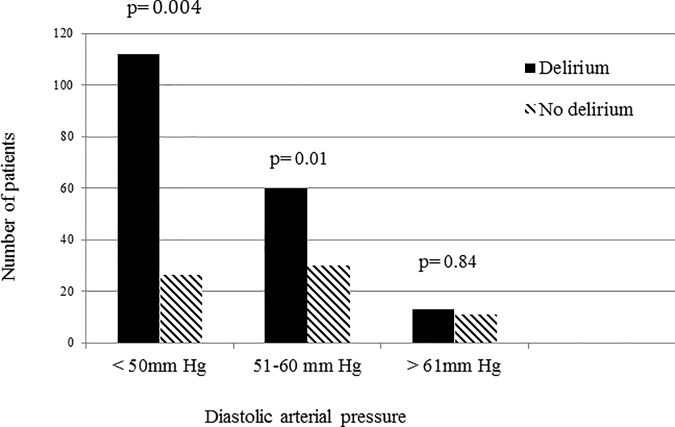
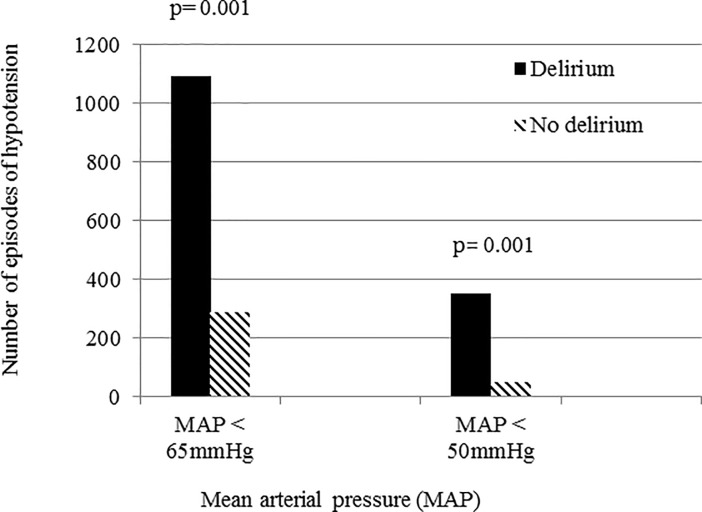
The pathogenesis of delirium in critically ill patients is multifactorial. How hypotension and hypoxemia affect brain function and whether they can promote delirium remains unclear. A high cumulative positive fluid balance may also have a negative effect on brain function and promote delirium. We hypothesized that delirium would be more likely to develop in patients with low systemic arterial pressure, hypoxemia and a higher positive fluid balance, and investigated these associations in a prospective observational cohort study in patients with shock. After initial resuscitation, episodes of hypotension, defined as a mean arterial pressure (MAP) <65 mmHg or diastolic pressure <60 mmHg, and hypoxemia, defined as peripheral oxygen saturation (SpO2) <90% for more than one minute or any arterial oxygen concentration (PaO2) <90 mmHg, were recorded during the first 5 days of the ICU stay. Fluid balance was evaluated daily and the 5-day cumulative fluid balance recorded. Delirium was assessed using the Confusion Assessment Method for the ICU. A total of 252 patients were admitted with shock during the study period; 185 (73%) developed delirium. Patients who developed delirium also had more episodes of hypotension with a low MAP (p = 0.013) or diastolic pressure (p = 0.018) during the first five days of the ICU stay than those who did not. Patients with a higher cumulative fluid balance during the same period were also more likely to develop delirium (p = 0.01); there was no significant difference in the occurrence of hypoxemia between groups. Joint modeling, combining a linear-mixed model and an adjusted Cox survival model showed that low diastolic pressure (alpha effect = -0.058±0.0013, p = 0.043) and a positive cumulative fluid balance (alpha effect = 0.04±0.003, p = 0.021) were independently associated with delirium. In conclusion, low diastolic pressure and a cumulative positive fluid balance but not hypoxemia were independently associated with development of delirium in patients with shock.
在危重病患者中,谵妄的发病机制是多因素的。低血压和低氧血症如何影响脑功能,以及它们是否能促进谵妄,目前尚不清楚。高累积正液体平衡也可能对脑功能产生负面影响,促进谵妄。我们假设在低血压、低氧血症和更高的正液体平衡的患者中,谵妄更有可能发生,并在休克患者的前瞻性观察队列研究中对此进行了研究。在最初的复苏后,在 ICU 入住的前 5 天内记录了低血压发作,定义为平均动脉压 (MAP) <65mmHg 或舒张压 <60mmHg,以及低氧血症,定义为外周血氧饱和度 (SpO2) <90%超过一分钟或任何动脉氧浓度 (PaO2) <90mmHg。每天评估液体平衡,并记录 5 天的累积液体平衡。使用 ICU 意识模糊评估法评估谵妄。在研究期间,共有 252 名患者因休克入院;185 名(73%)发生谵妄。发生谵妄的患者在 ICU 入住的前 5 天内也有更多的低血压发作,MAP 较低(p=0.013)或舒张压较低(p=0.018)。同期累积液体平衡较高的患者也更容易发生谵妄(p=0.01);两组之间缺氧的发生率没有显著差异。联合建模,将线性混合模型和调整后的 Cox 生存模型结合起来,显示舒张压低(alpha 效应=-0.058±0.0013,p=0.043)和正累积液体平衡(alpha 效应=0.04±0.003,p=0.021)与谵妄的发生独立相关。总之,低血压和累积正液体平衡,而不是低氧血症,与休克患者谵妄的发生独立相关。