Amore Dario, Imitazione Pasquale, Palma Albina, Casazza Dino, Scaramuzzi Roberto, Di Natale Davide, Molino Antonio, Curcio Carlo
Division of Thoracic Surgery, Monaldi Hospital, Leonardo Bianchi Street, 80131, Naples, Italy.
Department of Respiratory Diseases, Division of Pneumology, University of Naples Federico II, Monaldi Hospital, Leonardo Bianchi Street, 80131, Naples, Italy.
Int J Surg Case Rep. 2018;51:272-274. doi: 10.1016/j.ijscr.2018.09.006. Epub 2018 Sep 12.
Most hamartomas are located peripherally in the lung parenchyma and are rarely identified as an endobronchial lesion. Clinically patients with an endobronchial hamartoma are often symptomatic and may present with various symptoms including: fever, wheezing, hemoptysis and obstructive pneumonia.
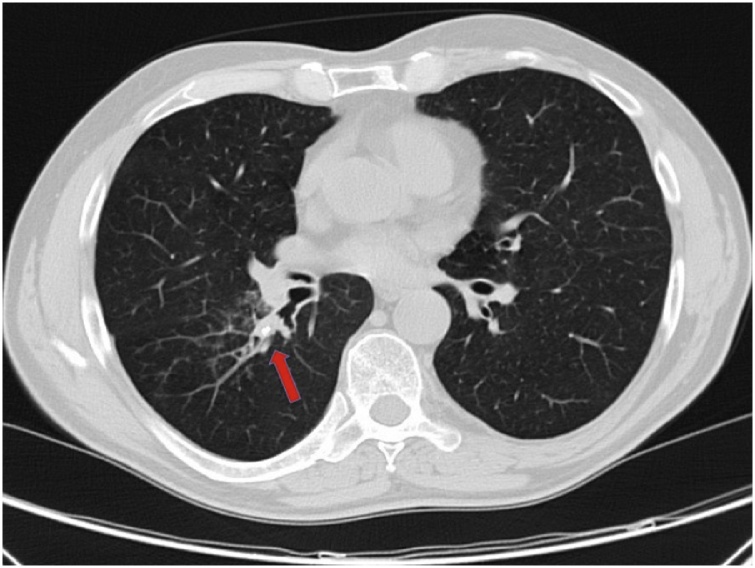
A 68-year-old man presented with complaints of fever and cough for 1 month. Chest X-ray revealed a right infrahilar density, which on chest CT was found to be a lesion obstructing the superior segmental bronchus of the right lower lobe and extending outside of the bronchus. A round rubbery mass obstructing the same segmental bronchus was noticed during bronchoscopy and endoscopic biopsy yielded a pathological diagnosis of hamartoma.
Bronchoscopy is most helpful in diagnosis and management of endobronchial hamartomas but if the lung distal to the obstruction is irreversibly damaged or imaging studies suggest that tumor extends outside of the bronchus, pulmonary segmentectomy, lobar resection or even pneumonectomy may be indicated.
When a benign tumor of the lung, as endobronchial hamartoma, is located in a segmental bronchus and presents extrabronchial spread, we recommend to perform a parenchymal-sparing surgical resection. In this case surgical team, however, should keep in mind, due to difficult individual dissection of the segmental bronchovascular elements, the possibility of conversion from VATS (video-assisted thoracic surgery) to open thoracotomy.
大多数错构瘤位于肺实质周边,很少被识别为支气管内病变。临床上,支气管内错构瘤患者常出现症状,可能表现为多种症状,包括发热、喘息、咯血和阻塞性肺炎。
一名68岁男性因发热和咳嗽1个月就诊。胸部X线显示右下肺门下方有密度影,胸部CT发现是一个阻塞右下叶上段支气管并延伸至支气管外的病变。支气管镜检查时发现一个圆形橡胶样肿物阻塞同一节段支气管,内镜活检病理诊断为错构瘤。
支气管镜检查对支气管内错构瘤的诊断和治疗最有帮助,但如果阻塞远端的肺组织已发生不可逆损伤或影像学检查提示肿瘤延伸至支气管外,则可能需要进行肺段切除术、肺叶切除术甚至全肺切除术。
当肺部良性肿瘤,如支气管内错构瘤,位于节段支气管并出现支气管外扩散时,我们建议进行保留实质的手术切除。然而,在这种情况下,手术团队应牢记,由于节段支气管血管结构的个体解剖困难,存在从电视辅助胸腔镜手术(VATS)转为开胸手术的可能性。