Department of Neurology, St Olavs Hospital, Trondheim University Hospital, Trondheim, Norway.
Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway.
Brain Behav. 2018 Oct;8(10):e01113. doi: 10.1002/brb3.1113. Epub 2018 Sep 21.
Accurate and reliable clinical and radiological predictors of intracerebral hemorrhage (ICH) outcomes are needed to optimize treatment of ICH. The aim of this study was to investigate functional outcome and identify predictors of severe disability or death following ICH.
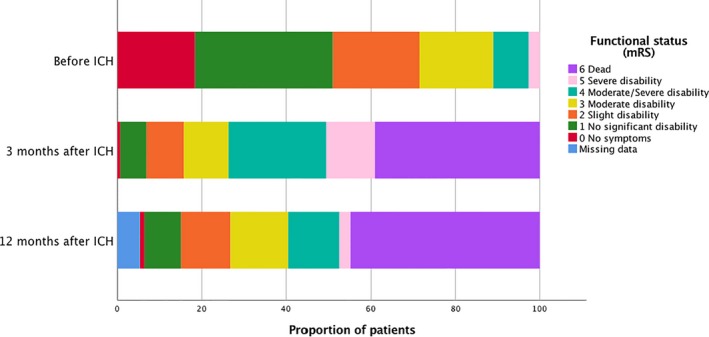
Retrospective population-based study of spontaneous ICH. Clinical and radiological data were obtained from electronic medical records, and functional outcome estimated using the modified Rankin Scale (mRS) before ICH and at 3 and 12 months after ICH.
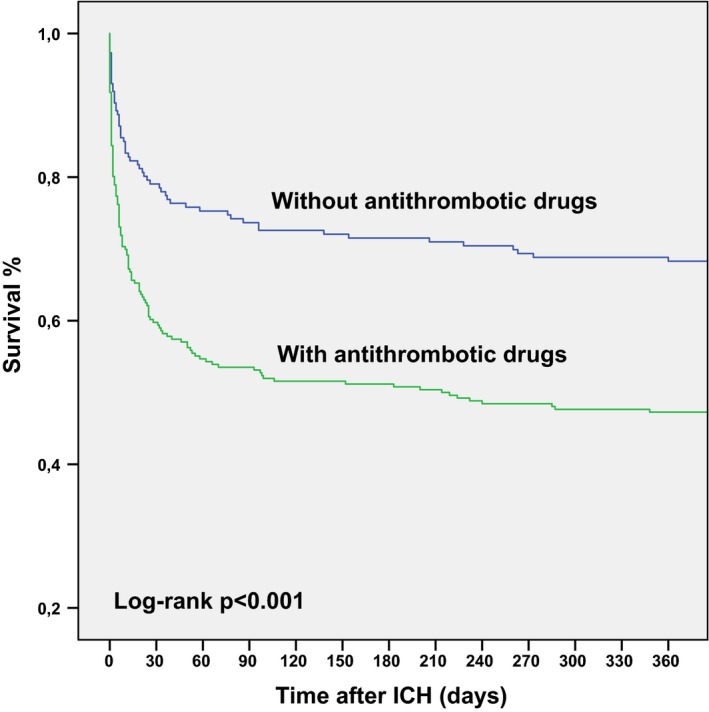
Four hundred and fifty-two patients were included (mean age 74.8 years, 45.6% females). Proportion of fatal outcome at 1 week was 22.1%, at 3 months 39.2%, and at 12 months 44.9%. Median mRS score before the ICH was 1 (interquartile range [IQR] 2); for survivors at 3 months, it was 5 (IQR 3); and at 12 months, it was 3 (IQR 2). Independent predictors of severe disability (mRS of 5) or death (mRS of 6) were use of oral antithrombotic drugs (OR 2.2, 95% CI 1.3-3.8, p = 0.04), mRS score before the ICH (OR 1.8, 95% CI 1.4-2.2, p < 0.001), Glasgow Coma Scale (GCS) on admission (OR 8.3, 95% CI 3.5-19.7, p < 0.001), hematoma volume >60 ml (OR 4.5, 05% CI 2.0-10.2, p < 0.001), and intraventricular hematoma extension (OR 1.8, 95% CI 0.8-4.2, p < 0.001).
Intracerebral hemorrhage is associated with high mortality, and more than one third of survivors end up with severe disability or death 3 months later. Predictors of severe disability or death were use of oral antithrombotic drugs, functional disability prior to ICH, low GCS on admission, larger hematoma volume, and intraventricular hematoma extension.
需要准确可靠的临床和影像学指标来预测脑出血(ICH)的结局,以优化 ICH 的治疗。本研究旨在探讨功能结局,并确定ICH 后发生严重残疾或死亡的预测因素。
对自发性 ICH 进行回顾性基于人群的研究。从电子病历中获取临床和影像学数据,并在 ICH 前、ICH 后 3 个月和 12 个月使用改良 Rankin 量表(mRS)评估功能结局。
共纳入 452 例患者(平均年龄 74.8 岁,45.6%为女性)。ICH 后 1 周的病死率为 22.1%,3 个月时为 39.2%,12 个月时为 44.9%。ICH 前 mRS 中位数为 1(四分位距 [IQR] 2);对于幸存者,3 个月时为 5(IQR 3),12 个月时为 3(IQR 2)。严重残疾(mRS 5)或死亡(mRS 6)的独立预测因素为口服抗血栓药物的使用(OR 2.2,95%CI 1.3-3.8,p=0.04)、ICH 前 mRS 评分(OR 1.8,95%CI 1.4-2.2,p<0.001)、入院时格拉斯哥昏迷量表(GCS)评分(OR 8.3,95%CI 3.5-19.7,p<0.001)、血肿体积>60ml(OR 4.5,95%CI 2.0-10.2,p<0.001)和脑室内血肿扩展(OR 1.8,95%CI 0.8-4.2,p<0.001)。
ICH 死亡率高,超过三分之一的幸存者在 3 个月后出现严重残疾或死亡。严重残疾或死亡的预测因素包括口服抗血栓药物的使用、ICH 前功能障碍、入院时 GCS 评分较低、较大的血肿体积和脑室内血肿扩展。