Rovere-Querini Patrizia, Canti Valentina, Erra Roberta, Bianchi Esperia, Slaviero Giorgio, D'Angelo Armando, Rosa Susanna, Candiani Massimo, Castiglioni Maria Teresa
Division of Immunology, Transplantation and Infectious diseases, IRCCS Ospedale San Raffaele.
Università Vita-Salute San Raffaele.
Medicine (Baltimore). 2018 Oct;97(40):e12584. doi: 10.1097/MD.0000000000012584.
Hypercoagulability and pregnancy morbidity are hallmarks of the antiphospholipid syndrome (APS). Catastrophic antiphospholipid syndrome (CAPS) is a potentially life-threatening omplication of APS, with widespread acute thrombotic microangiopathy (TMA) that can be precipitated by pregnancy and delivery and result in multiorgan damage. Unrestrained activation of the complement cascade is involved, favoring endothelial activation, tissue factor expression by leukocytes, and platelet aggregation. The complement block, which interrupts this amplification cycle, could prevent CAPS in patients with early TMA who face precipitating events.
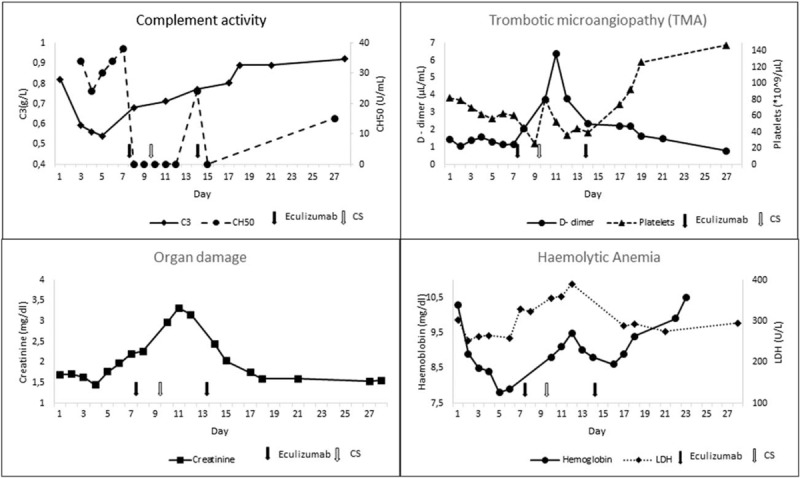
We present a nulliparous pregnant woman with APS at the 30 week of gestation who has developed thrombocytopenia, intravascular hemolysis, elevated creatinine, proteinuria, and hematuria.
These featurs were compatible with the diagnosis of CAPS. Consensually, serum C3 protein levels were rapidly decreasing, reflecting complement consumption.
She was treated with eculizumab, a humanized monoclonal antibody against C5 that prevents the formation of the complement membrane attack complex.
Laboratory parameters improved and the patient did not develop thrombosis or detectable organ/tissue damage. The patient safely delivered by cesarean section at week 32 of gestation a healthy 1640 g male infant. After 5 days, she received additional eculizumab, with complete resolution of the clinical condition. Low complement activity was detectable in the infant blood for a week after delivery. No infectious complication occurred.
Inhibition of the terminal complement activation is safe and might be effective in patients with APS developing early TMA, enabling safe delivery and preventing thrombotic events both in the mother and in the newborn.
高凝状态和妊娠并发症是抗磷脂综合征(APS)的特征。灾难性抗磷脂综合征(CAPS)是APS的一种潜在危及生命的并发症,伴有广泛的急性血栓性微血管病(TMA),可由妊娠和分娩诱发,并导致多器官损伤。补体级联反应的不受控制激活参与其中,促进内皮细胞激活、白细胞组织因子表达和血小板聚集。补体阻断可中断这一放大循环,对于面临诱发事件的早期TMA患者,可能预防CAPS。
我们报告一名妊娠30周的未生育孕妇,患有APS,出现了血小板减少、血管内溶血、肌酐升高、蛋白尿和血尿。
这些特征符合CAPS的诊断。经共识,血清C3蛋白水平迅速下降,反映了补体消耗。
她接受了依库珠单抗治疗,这是一种针对C5的人源化单克隆抗体,可防止补体膜攻击复合物的形成。
实验室指标改善,患者未发生血栓形成或可检测到的器官/组织损伤。患者在妊娠32周时通过剖宫产安全分娩出一名健康的1640克男婴。5天后,她再次接受依库珠单抗治疗,临床状况完全缓解。婴儿出生后一周内,其血液中可检测到低补体活性。未发生感染性并发症。
抑制补体终末激活对发生早期TMA的APS患者是安全的,可能有效,可实现安全分娩并预防母亲和新生儿的血栓形成事件。