The National Institute for Health Research (NIHR) Health Protection Research Unit in Healthcare Associated Infections and Antimicrobial Resistance at University of Oxford, Oxford, United Kingdom.
Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom.
PLoS One. 2018 Nov 7;13(11):e0206860. doi: 10.1371/journal.pone.0206860. eCollection 2018.
Reporting of strategic healthcare-associated infections (HCAIs) to Public Health England is mandatory for all acute hospital trusts in England, via a web-based HCAI Data Capture System (HCAI-DCS).
Investigate the feasibility of automating the current, manual, HCAI reporting using linked electronic health records (linked-EHR), and assess its level of accuracy.
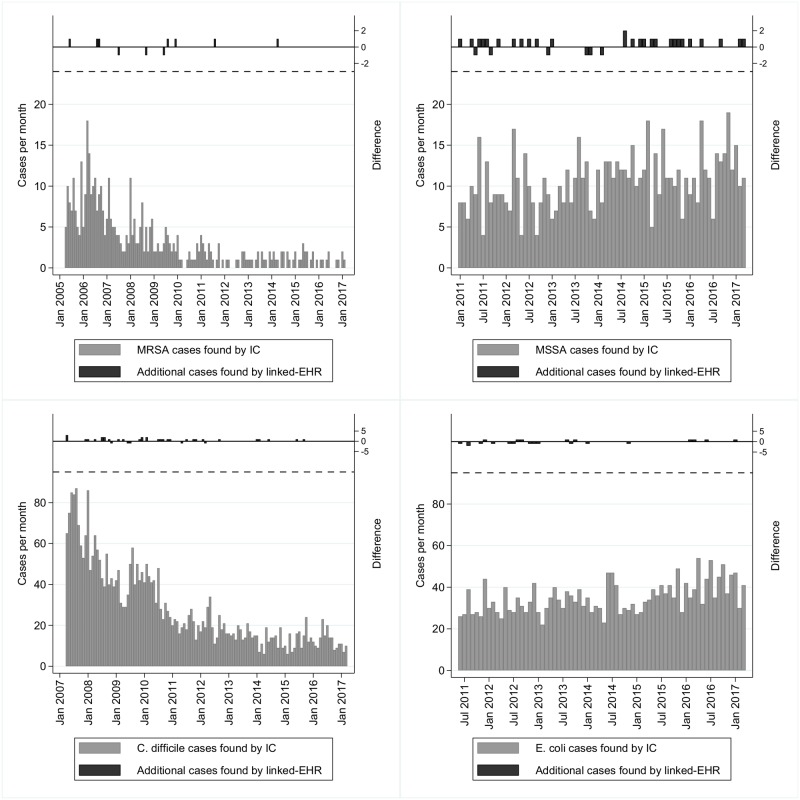
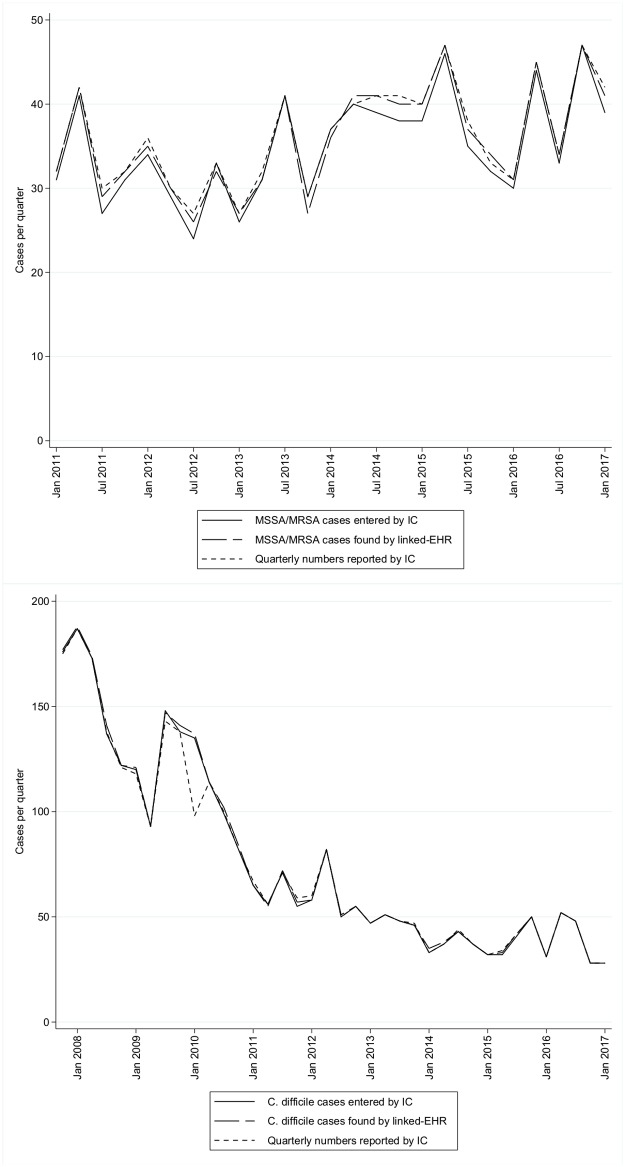
All data previously submitted through the HCAI-DCS by the Oxford University Hospitals infection control (IC) team for methicillin-resistant and methicillin-susceptible Staphylococcus aureus (MRSA, MSSA), Clostridium difficile, and Escherichia coli, through March 2017 were downloaded and compared to outputs created from linked-EHR, with detailed comparisons between 2013-2017.
Total MRSA, MSSA, E. coli and C. difficile cases entered by the IC team vs linked-EHR were 428 vs 432, 795 vs 816, 2454 vs 2450 and 3365 vs 3393 respectively. From 2013-2017, most discrepancies (32/37 (86%)) were likely due to IC recording errors. Patient and specimen identifiers were completed for >98% of cases by both methods, with very high agreement (>97%). Fields relating to the patient at the time the specimen was taken were complete to a similarly high level (>99% IC, >97% linked-EHR), and agreement was fairly good (>80%) except for the main and treatment specialties (57% and 54% respectively) and the patient category (55%). Optional, organism-specific data-fields were less complete, by both methods. Where comparisons were possible, agreement was reasonably high (mostly 70-90%).
Basic factual information, such as demographic data, is almost-certainly better automated, and many other data fields can potentially be populated successfully from linked-EHR. Manual data collection is time-consuming and inefficient; automated electronic data collection would leave healthcare professionals free to focus on clinical rather than administrative work.
英格兰所有急症医院信托机构都必须通过基于网络的战略卫生保健相关感染(HCAI)数据采集系统(HCAI-DCS)向英国公共卫生署报告战略卫生保健相关感染。
调查使用电子病历(linked-EHR)自动完成当前手动 HCAI 报告的可行性,并评估其准确性。
牛津大学医院感染控制(IC)团队通过 HCAI-DCS 提交的所有数据(2017 年 3 月前)均已下载,并与 linked-EHR 生成的输出进行比较,2013-2017 年进行了详细比较。
IC 团队与 linked-EHR 录入的总 MRSA、MSSA、大肠杆菌和艰难梭菌病例数分别为 428 与 432、795 与 816、2454 与 2450、3365 与 3393。2013-2017 年,大多数差异(32/37(86%))可能是由于 IC 记录错误。两种方法的患者和标本标识符的完成率均超过 98%,且非常一致(>97%)。与标本采集时患者相关的字段完成率也很高(>99%的 IC、>97%的 linked-EHR),一致性也相当好(>80%),除主要和治疗专业(分别为 57%和 54%)和患者类别(55%)外。两种方法的可选、特定于生物体的数据字段的完整性均较差。在可以进行比较的地方,一致性相当高(大多为 70-90%)。
基本事实信息(如人口统计数据)几乎肯定可以更好地自动化,许多其他数据字段也可以从 linked-EHR 中成功填充。手动数据收集既耗时又效率低下;自动电子数据收集将使医疗保健专业人员能够自由地专注于临床工作而不是行政工作。