Nakajima Hiroyuki, Takazawa Akitoshi, Yoshitake Akihiro, Tochii Masato, Tokunaga Chiho, Hayashi Jun, Izumida Hiroaki, Kaneyuki Daisuke, Asakura Toshihisa, Iguchi Atsushi
Department of Cardiovascular Surgery, Saitama Medical University, International Medical Center, 1397-1 Yamane Hidaka, Saitama, 350-1298, Japan.
J Cardiothorac Surg. 2018 Nov 22;13(1):121. doi: 10.1186/s13019-018-0806-6.
The aim of this study was to delineate impacts of percutaneous coronary intervention (PCI), flow demand, and status of myocardium on graft flow.
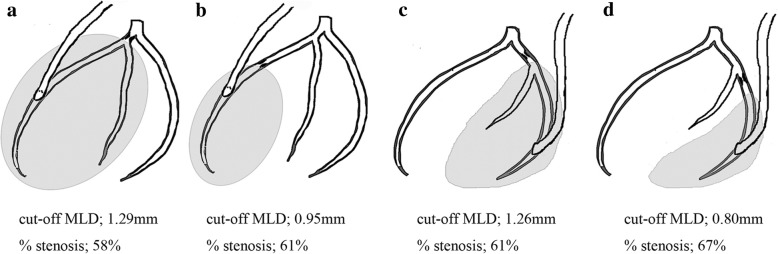
We retrospectively assessed 736 individual coronary artery bypass grafts that had been created as the sole bypass graft for a vascular region in 405 patients. The grafts comprised 334 internal thoracic artery (ITA) to left anterior descending (LAD), 129 ITA and 65 saphenous vein grafts (SVG) to left circumflex (LCX), and 142 gastroepiploic artery (GEA) and 66 SVG to right coronary artery (RCA). Minimal luminal diameter, size of revascularized area, history of myocardial infarction, and PCI in the relevant area were examined to determine whether these factors are associated with flow insufficiency (FI), which was defined as ≤ 20 mL/min.
FI developed in 123/736 grafts (16.7%) and correlated significantly with stenosis in the distal portion (23.0% vs. 12.8%, p = 0.0003). Prior myocardial infarction significantly correlated with FI in GEA-RCA (p = 0.002) and ITA-LCX grafts (p = 0.04). There was a history of PCI to the LAD (PCI group) in 54 ITA to LAD bypass grafts (16.2%), whereas the remaining 280 had no history of PCI to the LAD (no-PCI group). Graft flow was significantly greater in the no-PCI than in the PCI group (53 ± 29 vs. 42 ± 27; p = 0.006). The incidences of FI and graft failure were significantly higher in the PCI than the no-PCI group (22.2%, vs. 8.2%; p = 0.003; 9.2% vs. 1.8%; p = 0.003, respectively).
Prior PCI has a negative impact on graft flow. The influences of small revascularized area, myocardial infarction, and PCI are greater, necessitating consideration of factors associated with flow demand or microvasculature when planning revascularization.
本研究的目的是阐明经皮冠状动脉介入治疗(PCI)、血流需求和心肌状态对移植血管血流的影响。
我们回顾性评估了405例患者中作为血管区域唯一旁路移植术创建的736条个体冠状动脉旁路移植血管。这些移植血管包括334条左胸廓内动脉(ITA)至左前降支(LAD)、129条ITA和65条大隐静脉移植血管(SVG)至左旋支(LCX),以及142条胃网膜动脉(GEA)和66条SVG至右冠状动脉(RCA)。检查最小管腔直径、血运重建区域大小、心肌梗死病史以及相关区域的PCI情况,以确定这些因素是否与血流不足(FI)相关,FI定义为≤20 mL/min。
123/736条移植血管(16.7%)出现FI,且与远端狭窄显著相关(23.0%对12.8%,p = 0.0003)。既往心肌梗死与GEA-RCA(p = 0.002)和ITA-LCX移植血管中的FI显著相关(p = 0.04)。54条ITA至LAD旁路移植血管(16.2%)存在LAD的PCI病史(PCI组),而其余280条无LAD的PCI病史(无PCI组)。无PCI组的移植血管血流显著大于PCI组(53±29对42±27;p = 0.006)。PCI组的FI和移植血管失败发生率显著高于无PCI组(分别为22.2%对8.2%;p = 0.003;9.2%对1.8%;p = 0.003)。
既往PCI对移植血管血流有负面影响。血运重建区域小、心肌梗死和PCI的影响更大,在规划血运重建时需要考虑与血流需求或微血管系统相关的因素。