Bottle Alex, Kim Dani, Aylin Paul P, Majeed F Azeem, Cowie Martin R, Hayhoe Benedict
Dr Foster Unit, Department of Primary Care and Public Health, Imperial College London, London, UK.
Department of Primary Care and Public Health, Imperial College London, London, UK.
Open Heart. 2018 Nov 10;5(2):e000935. doi: 10.1136/openhrt-2018-000935. eCollection 2018.
To describe associations between initial management of people presenting with heart failure (HF) symptoms in primary care, including compliance with the recommendations of the National Institute for Health and Care Excellence (NICE), and subsequent unplanned hospitalisation for HF and death.
This is a retrospective cohort study using data from general practices submitting records to the Clinical Practice Research Datalink. The cohort comprised patients diagnosed with HF during 2010-2013 and presenting to their general practitioners with breathlessness, fatigue or ankle swelling.
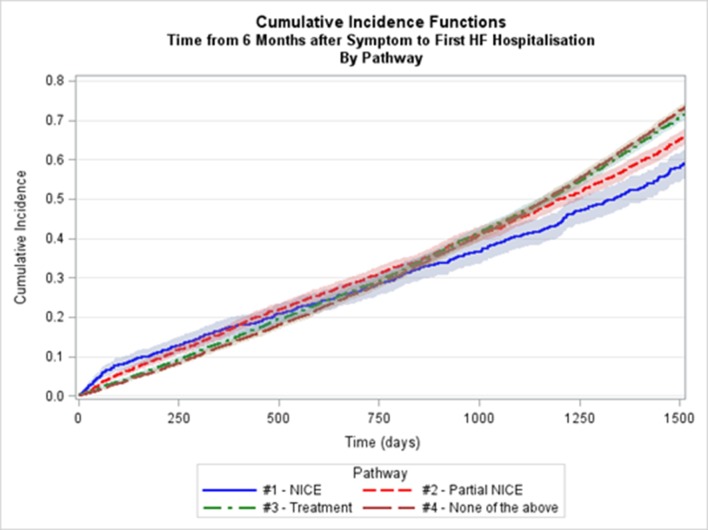
13 897 patients were included in the study. Within the first 6 months, only 7% had completed the NICE-recommended pathway; another 18.6% had followed part of it (B-type natriuretic peptide testing and/or echocardiography, or specialist referral). Significant differences in hazards were seen in unadjusted analysis in favour of full or partial completion of the NICE-recommended pathway. Covariate adjustment attenuated the relations with death much more than those for HF admission. Compared with patients placed on the NICE pathway, treatment with HF medications had an HR of 1.16 (95% CI 1.05 to 1.28, p=0.003) for HF admission and 1.03 (95% CI 0.90 to 1.17, p= 0.674) for death. Patients who partially followed the NICE pathway had similar hazards to those who completed it. Patients on no pathway had the highest hazard for HF admission at 1.30 (95% 1.18 to 1.43, p<0.001) but similar hazard for death.
Patients not put on at least some elements of the NICE-recommended pathway had significantly higher risk of HF admission but non-significant higher risk of death than other patients had.
描述初级保健中出现心力衰竭(HF)症状患者的初始管理情况(包括是否符合英国国家卫生与临床优化研究所(NICE)的建议)与随后因HF导致的非计划住院和死亡之间的关联。
这是一项回顾性队列研究,使用了向临床实践研究数据链提交记录的全科医疗数据。该队列包括2010年至2013年期间被诊断为HF并因气促、疲劳或脚踝肿胀就诊于全科医生的患者。
13897名患者纳入研究。在最初6个月内,仅7%的患者完成了NICE推荐的流程;另有18.6%的患者遵循了其中部分流程(B型利钠肽检测和/或超声心动图检查,或专科转诊)。在未调整分析中,观察到显著的风险差异,支持完全或部分完成NICE推荐流程。协变量调整对与死亡的关系的减弱程度远大于对HF入院的关系。与遵循NICE流程的患者相比,使用HF药物治疗的患者因HF入院的风险比为1.16(95%置信区间1.05至1.28,p = 0.003),因死亡的风险比为1.03(95%置信区间0.90至1.17,p = 0.674)。部分遵循NICE流程的患者与完成该流程的患者风险相似。未遵循任何流程的患者因HF入院的风险最高,为1.30(95%置信区间1.18至1.43,p<0.001),但因死亡的风险相似。
未遵循NICE推荐流程中至少某些环节的患者,其HF入院风险显著高于其他患者,但死亡风险虽有升高但无统计学意义。