Division of Nephrology, Department of Medicine, and Departments of.
Institute for Clinical Evaluative Sciences, Ontario, Canada.
Clin J Am Soc Nephrol. 2019 Jan 7;14(1):17-26. doi: 10.2215/CJN.07490618. Epub 2018 Dec 11.
Regulatory agencies warn about the risk of AKI with levetiracetam use on the basis of information from case reports. We conducted this study to determine whether new levetiracetam use versus nonuse is associated with a higher risk of AKI.
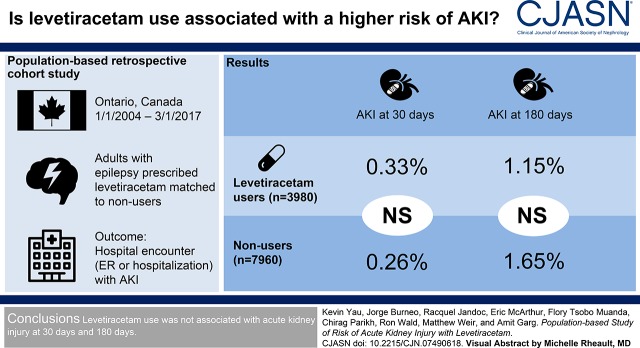
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: This was a population-based retrospective cohort study of adults with epilepsy in Ontario, Canada. Patients who received a new outpatient prescription for levetiracetam between January 1, 2004 and March 1, 2017 were matched to two nonusers on stage of CKD, recorded seizure in the prior 90 days, and logit of a propensity score for levetiracetam use. The primary outcome was a hospital encounter (emergency department visit or hospitalization) with AKI within 30 days of cohort entry. Secondary outcomes were AKI within 180 days and change in the concentration of serum creatinine. We assessed the primary outcome using health care diagnosis codes. We evaluated the change in the concentration of serum creatinine in a subpopulation with laboratory measurements.
We matched 3980 levetiracetam users to 7960 nonusers (mean age 55 years, 51% women). Levetiracetam use was not significantly associated with a higher risk of AKI within 30 days (13 [0.33%] events in levetiracetam users and 21 [0.26%] events in nonusers [odds ratio, 1.24; 95% confidence interval, 0.62 to 2.47]). Similarly, there was no significant association with AKI within 180 days (odds ratio, 0.70; 95% confidence interval, 0.43 to 1.13). The change in the concentration of serum creatinine did not significantly differ between levetiracetam users and nonusers.
In this population-based study levetiracetam use was not associated with a higher risk of AKI.
This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2018_12_11_Yau_Podcast.mp3.
监管机构基于病例报告的信息警告使用左乙拉西坦可能会导致 AKI。我们进行这项研究是为了确定新使用左乙拉西坦与不使用相比是否会增加 AKI 的风险。
设计、设置、参与者和测量方法:这是一项基于加拿大安大略省癫痫患者的人群回顾性队列研究。2004 年 1 月 1 日至 2017 年 3 月 1 日期间,接受左乙拉西坦新门诊处方的患者与在 CKD 阶段、记录在过去 90 天内有癫痫发作且左乙拉西坦使用倾向评分的逻辑对数相匹配的两名非使用者相匹配。主要结局是队列入组后 30 天内发生 AKI 的医院就诊(急诊就诊或住院)。次要结局是在 180 天内发生 AKI 和血清肌酐浓度的变化。我们使用医疗保健诊断代码评估主要结局。我们在有实验室测量的亚人群中评估了血清肌酐浓度的变化。
我们将 3980 名左乙拉西坦使用者与 7960 名非使用者相匹配(平均年龄 55 岁,51%为女性)。左乙拉西坦的使用与 30 天内 AKI 的发生风险无显著相关性(左乙拉西坦使用者中有 13 例[0.33%],非使用者中有 21 例[0.26%][比值比,1.24;95%置信区间,0.62 至 2.47])。同样,180 天内 AKI 也无显著相关性(比值比,0.70;95%置信区间,0.43 至 1.13)。左乙拉西坦使用者与非使用者的血清肌酐浓度变化无显著差异。
在这项基于人群的研究中,左乙拉西坦的使用与 AKI 的风险增加无关。
本文包含播客链接:https://www.asn-online.org/media/podcast/CJASN/2018_12_11_Yau_Podcast.mp3。