Eskandary Farsad, Dürr Michael, Budde Klemens, Doberer Konstantin, Reindl-Schwaighofer Roman, Waiser Johannes, Wahrmann Markus, Regele Heinz, Spittler Andreas, Lachmann Nils, Firbas Christa, Mühlbacher Jakob, Bond Gregor, Halloran Philipp F, Chong Edward, Jilma Bernd, Böhmig Georg A
Division of Nephrology and Dialysis, Department of Medicine III, Medical University of Vienna, Währinger Gürtel 18-20, A-1090, Vienna, Austria.
Department of Nephrology, Charité University Medicine Berlin, Berlin, Germany.
Trials. 2019 Jan 11;20(1):37. doi: 10.1186/s13063-018-3158-6.
Late antibody-mediated rejection (ABMR) triggered by donor-specific antibodies (DSA) is a cardinal cause of kidney allograft dysfunction and loss. Diagnostic criteria for this rejection type are well established, but effective treatment remains a major challenge. Recent randomized controlled trials (RCT) have failed to demonstrate the efficacy of widely used therapies, such as rituximab plus intravenous immunoglobulin or proteasome inhibition (bortezomib), reinforcing a great need for new therapeutic concepts. One promising target in this context may be interleukin-6 (IL-6), a pleiotropic cytokine known to play an important role in inflammation and adaptive immunity.
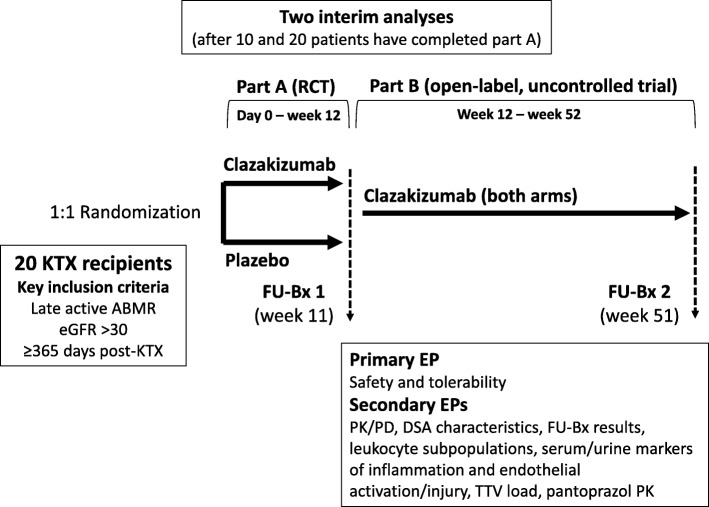
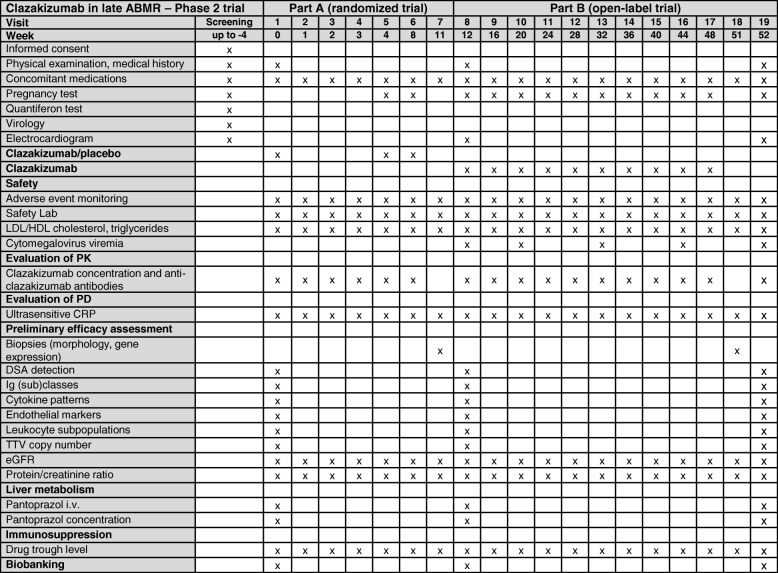
This investigator-driven RCT was designed to assess the safety and efficacy of clazakizumab, a genetically engineered humanized monoclonal antibody directed against IL-6. The study will include 20 DSA-positive kidney allograft recipients diagnosed with ABMR ≥ 365 days after transplantation. Participants will be recruited at two study sites in Austria and Germany (Medical University of Vienna; Charité University Medicine Berlin). First, patients will enter a three-month double-blind RCT (1,1 randomization, stratification according to ABMR phenotype and study site) and will receive either clazakizumab (subcutaneous administration of 25 mg in monthly intervals) or placebo. In a second open-label part of the trial (months 4-12), all patients will receive clazakizumab at 25 mg every month. The primary endpoint is safety and tolerability. Secondary endpoints are the pharmacokinetics and pharmacodynamics of clazakizumab, its effect on drug metabolism in the liver, DSA characteristics, morphological ABMR lesions and molecular gene expression patterns in three- and 12-month protocol biopsies, serum/urinary biomarkers of inflammation and endothelial activation/injury, Torque Teno viral load as a measure of overall immunosuppression, kidney function, urinary protein excretion, as well as transplant and patient survival.
Currently, there is no treatment proven to be effective in halting the progression of late ABMR. Based on the hypothesis that antagonizing the effects of IL-6 improves the outcome of DSA-positive late ABMR by counteracting DSA-triggered inflammation and B cell/plasma cell-driven alloimmunity, we suggest that our trial has the potential to provide proof of concept of a novel treatment of this type of rejection.
ClinicalTrials.gov, NCT03444103 . Registered on 23 February 2018 (retrospective registration).
由供体特异性抗体(DSA)引发的迟发性抗体介导排斥反应(ABMR)是肾移植功能障碍和丧失的主要原因。这种排斥反应类型的诊断标准已明确确立,但有效治疗仍然是一项重大挑战。近期的随机对照试验(RCT)未能证明广泛使用的疗法(如利妥昔单抗加静脉注射免疫球蛋白或蛋白酶体抑制(硼替佐米))的疗效,这凸显了对新治疗理念的迫切需求。在这种情况下,一个有前景的靶点可能是白细胞介素-6(IL-6),一种已知在炎症和适应性免疫中起重要作用的多效性细胞因子。
这项由研究者发起的RCT旨在评估克拉扎珠单抗(一种针对IL-6的基因工程人源化单克隆抗体)的安全性和疗效。该研究将纳入20名移植后≥365天被诊断为ABMR的DSA阳性肾移植受者。参与者将在奥地利和德国的两个研究地点招募(维也纳医科大学;柏林夏里特大学医学中心)。首先,患者将进入为期三个月的双盲RCT(1:1随机分组,根据ABMR表型和研究地点分层),并将接受克拉扎珠单抗(每月皮下注射25mg)或安慰剂。在试验的第二个开放标签部分(第4至12个月),所有患者将每月接受25mg克拉扎珠单抗。主要终点是安全性和耐受性。次要终点包括克拉扎珠单抗的药代动力学和药效学、其对肝脏药物代谢的影响、DSA特征、三个月和十二个月方案活检中的形态学ABMR病变和分子基因表达模式、炎症和内皮激活/损伤的血清/尿液生物标志物、作为总体免疫抑制指标的细小病毒载量、肾功能、尿蛋白排泄以及移植和患者生存率。
目前,尚无经证实能有效阻止晚期ABMR进展的治疗方法。基于拮抗IL-6的作用可通过抵消DSA引发的炎症和B细胞/浆细胞驱动的同种免疫来改善DSA阳性晚期ABMR结局的假设,我们认为我们的试验有潜力为这种类型的排斥反应的新治疗方法提供概念验证。
ClinicalTrials.gov,NCT03444103。于2018年2月23日注册(追溯注册)。