Aix-Marseille Univ, School of medicine - La Timone Medical Campus, EA 3279 CEReSS - Health Service Research and Quality of Life Center, |27 bd Jean Moulin cedex 05, F-13385, Marseille, France.
Réanimation, Clinique Ambroise Paré, Neuilly/Seine, France.
Health Qual Life Outcomes. 2019 Feb 7;17(1):29. doi: 10.1186/s12955-019-1101-5.
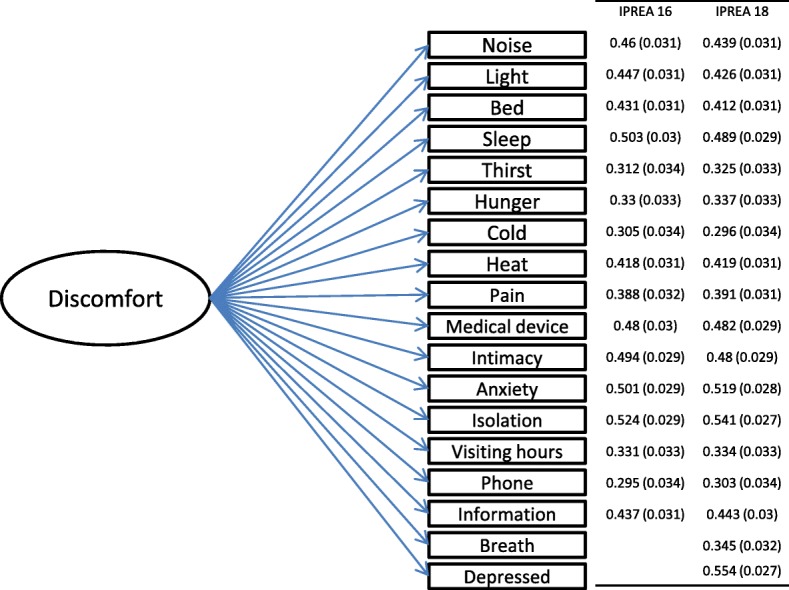
We reported the validation of the 18-item version of the 'Inconforts des Patients de REAnimation (IPREA)' questionnaire that includes 2 new items exploring feeling depressed and shortness of breath during an intensive care unit (ICU) stay.
The validation process was integrated in a multicenter, cluster-randomized, controlled, two-parallel group study built to assess the effectiveness of a tailored multicomponent program for reducing self-perceived discomfort in the ICU. All patients aged 18 years or older who survived an ICU stay of 3 calendar days or more were eligible for inclusion. Data collection included demographics (sex, age), type of admission (medical and surgical), health status scores at admission (Knaus score and McCabe index, Simplified Acute Physiology Score (SAPS) II), specific ICU therapeutics such as mechanical ventilation (MV), noninvasive ventilation (NIV), use of vasopressors, or renal replacement therapy (RRT), and ICU stay duration.
A total of 994 patients were included. The initial structure of IPREA was confirmed using confirmatory factor analysis showing satisfactory fit (RMSEA at 0.042, CFI at 0.912). No multidimensional structure was identified, allowing the calculation of an overall discomfort score. The three highest discomforts were sleep deprivation, thirst, and perfusion lines and other devices, and the 3 lowest discomforts were limited visiting hours, hunger, and isolation. The overall discomfort score of the 18-item version of IPREA did not differ between men and women. Higher age was significantly correlated with a lower overall discomfort score. While MV was not linked to self-reported discomfort, patients treated by NIV reported higher overall discomfort scores than patients not treated by NIV.
The 18-item version of IPREA is easy to use and possesses satisfactory psychometric properties. The availability of a reliable and valid French questionnaire asking about patients' self-perceived ICU discomforts enables feedback from the health care team to be incorporated in a continuous quality health care improvement strategy.
clinicaltrial.gov NCT02442934 (registration date: May 18, 2015, retrospectively registered).
我们报道了包含 2 项新条目(ICU 住院期间感到抑郁和呼吸急促)的 18 项《再监护患者不适问卷》(IPREA)的验证过程。
该验证过程整合在一项多中心、集群随机、对照、平行分组研究中,旨在评估一种量身定制的多组分方案对减少 ICU 患者自我感知不适的效果。所有 ICU 住院时间≥3 天且存活的年龄≥18 岁的患者均符合纳入标准。数据收集包括人口统计学信息(性别、年龄)、入院类型(内科和外科)、入院时的健康状况评分(Knaus 评分和 McCabe 指数、简化急性生理学评分 II (SAPS II))、特定 ICU 治疗措施(如机械通气(MV)、无创通气(NIV)、血管加压药的使用或肾脏替代治疗(RRT))和 ICU 住院时间。
共纳入 994 例患者。使用验证性因子分析确认了 IPREA 的初始结构,显示出良好的拟合度(RMSEA 为 0.042,CFI 为 0.912)。未发现多维结构,允许计算总体不适评分。最不适的三个方面是睡眠剥夺、口渴和灌注线及其他设备,最不不适的三个方面是探视时间受限、饥饿和隔离。18 项 IPREA 总体不适评分在男性和女性之间没有差异。年龄较大与总体不适评分较低显著相关。虽然 MV 与自我报告的不适无关,但接受 NIV 治疗的患者的总体不适评分高于未接受 NIV 治疗的患者。
18 项 IPREA 易于使用,具有良好的心理测量学特性。提供一种可靠和有效的法语问卷,询问患者自我感知的 ICU 不适,使医护团队的反馈能够纳入持续质量医疗保健改进策略。
clinicaltrial.gov NCT02442934(注册日期:2015 年 5 月 18 日,回溯性注册)。