Department of Critical Care Medicine, Affiliated Hospital of Zunyi Medical College, Zunyi Medical College, 149 Dalian Road, Zunyi, 563000, Guizhou, China.
Department of Ultrasound, Linyi City People's Hospital, Linyi, 276000, Shandong, China.
BMC Infect Dis. 2019 Feb 11;19(1):139. doi: 10.1186/s12879-019-3790-0.
In the new Sepsis-3 definition, sepsis is defined as "life-threatening organ dysfunction due to a dysregulated host response to infection." We tested the predictive validity of the systematic inflammatory response syndrome (SIRS) criteria in patients in the Sepsis-3 cohort.
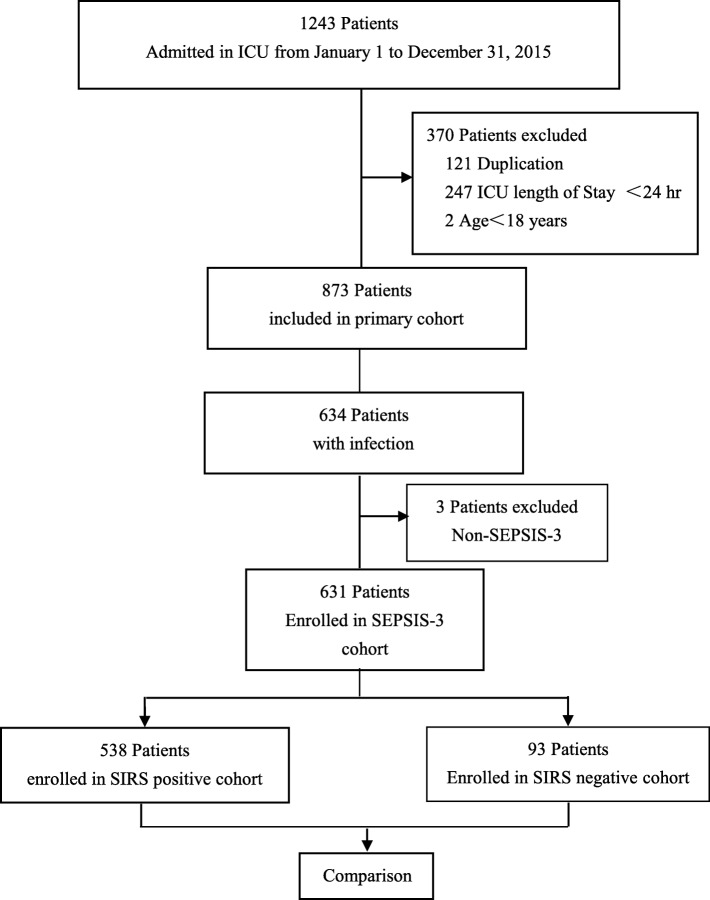
Among 1243 electronic health records from 1 January to 31 December 2015 at Sichuan University West China Hospital, we identified patients with sepsis and septic shock according to the Sepsis-3 definition and divided them into 2 subsets: SIRS-positive and SIRS-negative. We compared their characteristics and outcomes as well as the predictive validity of the SIRS criteria for in-hospital mortality.
Of the 1243 patients, 631 were enrolled. Among these, 538 (85.3%) patients had SIRS-positive sepsis or septic shock, 168 (31.2%) of whom died, and 93 (14.7%) had SIRS-negative sepsis or septic shock, 20 (21.5%) of whom died (p = 0.06). Over a 1-year period, these groups had similar characteristics and changes in mortality. Among patients of the Sepsis-3 cohort admitted to the intensive care unit, the predictive validity for in-hospital mortality was lower for the SIRS criteria (area under the receiver operating characteristic curve [AUROC], 0.53; 95% confidence interval [95% CI], 0.49-0.57) than for the sequential (sepsis-related) organ failure assessment (SOFA) criteria (AUROC, 0.70; 95% CI, 0.66-0.74; p ≤ 0.01 for both). The SIRS score had poor predictive validity for the risk of in-hospital mortality.
In this cohort study of the new Sepsis-3 definition, we found that the SIRS criteria are weaker than the SOFA criteria with respect to their predictive efficacy for in-hospital death.
在新的 Sepsis-3 定义中,败血症被定义为“由于宿主对感染的失调反应导致危及生命的器官功能障碍”。我们测试了系统性炎症反应综合征(SIRS)标准在 Sepsis-3 队列患者中的预测有效性。
在 2015 年 1 月 1 日至 12 月 31 日期间,我们从四川大学华西医院的 1243 份电子健康记录中确定了根据 Sepsis-3 定义诊断为败血症和败血症性休克的患者,并将他们分为 2 个子集:SIRS 阳性和 SIRS 阴性。我们比较了他们的特征和结局,以及 SIRS 标准对住院死亡率的预测准确性。
在 1243 名患者中,有 631 名患者入组。其中,538 名(85.3%)患者患有 SIRS 阳性败血症或败血症性休克,其中 168 名(31.2%)死亡,93 名(14.7%)患有 SIRS 阴性败血症或败血症性休克,其中 20 名(21.5%)死亡(p=0.06)。在 1 年期间,这些组的特征和死亡率变化相似。在 Sepsis-3 队列中入住重症监护病房的患者中,SIRS 标准对住院死亡率的预测准确性较低(接受者操作特征曲线下面积 [AUROC],0.53;95%置信区间 [95%CI],0.49-0.57)低于序贯(与败血症相关的)器官衰竭评估(SOFA)标准(AUROC,0.70;95%CI,0.66-0.74;p≤0.01)。SIRS 评分对住院死亡率的风险预测准确性较差。
在这项新的 Sepsis-3 定义的队列研究中,我们发现 SIRS 标准在预测住院死亡方面的预测效果弱于 SOFA 标准。