Rosenblatt Kathryn, Walker Keenan A, Goodson Carrie, Olson Elsa, Maher Dermot, Brown Charles H, Nyquist Paul
Department of Anesthesiology and Critical Care Medicine, 1466Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Department of Neurology, 1466Johns Hopkins University School of Medicine, Baltimore, MD, USA.
J Intensive Care Med. 2020 Dec;35(12):1453-1464. doi: 10.1177/0885066619828293. Epub 2019 Feb 13.
Impaired cerebral autoregulation and cerebral hypoperfusion may play a critical role in the high morbidity and mortality in patients with sepsis-associated encephalopathy (SAE). Bedside assessment of cerebral autoregulation may help individualize hemodynamic targets that optimize brain perfusion. We hypothesize that near-infrared spectroscopy (NIRS)-derived cerebral oximetry can identify blood pressure ranges that enhance autoregulation in patients with SAE and that disturbances in autoregulation are associated with severity of encephalopathy.
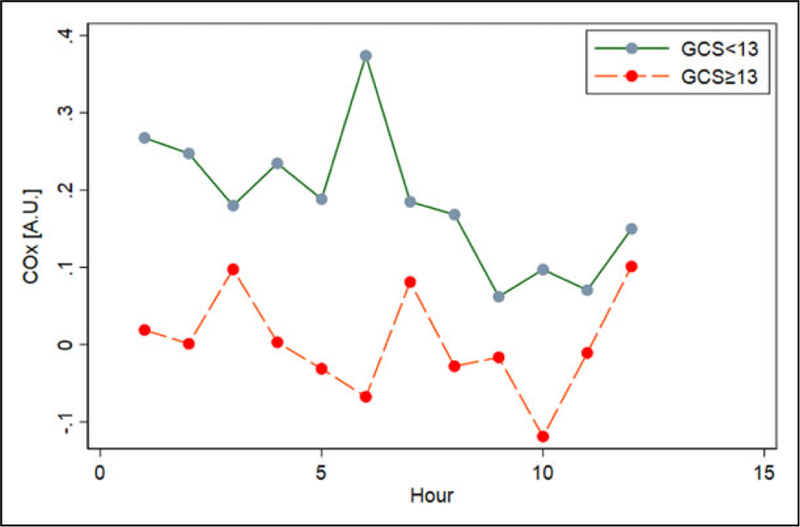
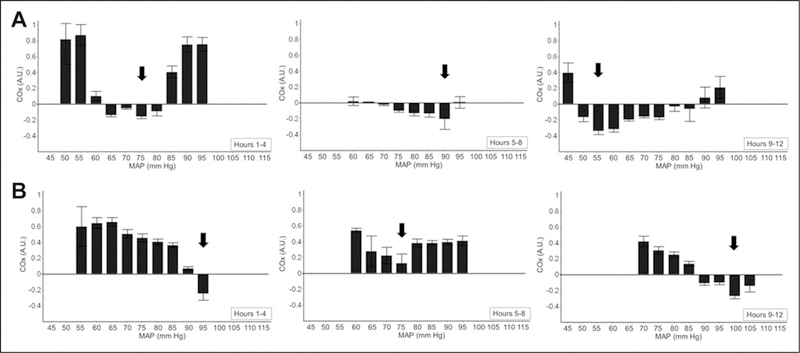
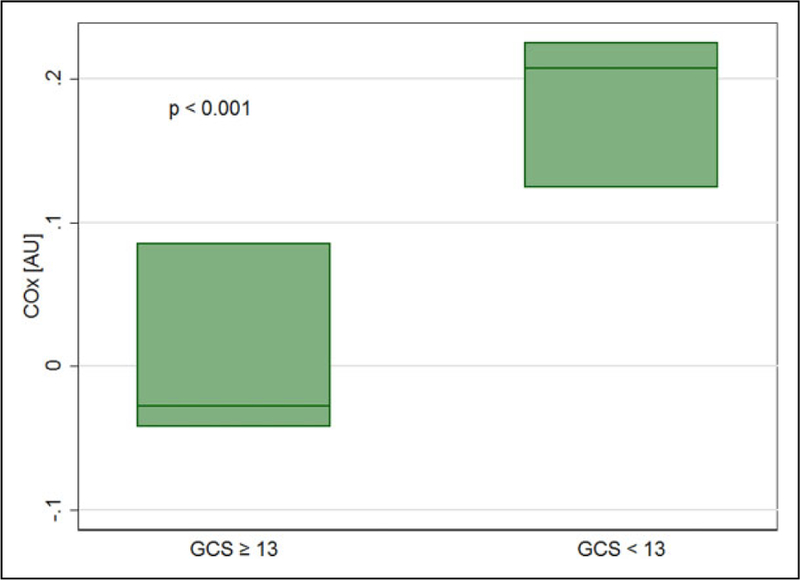
Adult patients with acute encephalopathy directly attributable to sepsis were followed using NIRS-based multimodal monitoring for 12 consecutive hours. We used the correlation in time between regional cerebral oxygen saturation and mean arterial pressure (MAP) to determine the cerebral oximetry index (COx) as a measure of cerebral autoregulation. Autoregulation curves were constructed for each patient with averaged COx values sorted by MAP in 3 sequential 4-hour periods; the optimal pressure (MAP), defined as the MAP associated with most robust autoregulation (lowest COx), was identified in each period. Severity of encephalopathy was measured with Glasgow coma scale (GCS).
Six patients with extracranial sepsis met the stringent criteria specified, including no pharmacological sedation or neurologic premorbidity. Optimal MAP was identified in all patients and ranged from 55 to 115 mmHg. Additionally, MAP varied within individual patients over time during monitoring. Disturbed autoregulation, based on COx, was associated with worse neurologic status (GCS < 13) both with and without controlling for age and severity of sepsis (adjusted odds ratio [OR]: 2.11; 95% confidence interval [CI]: 1.77-2.52; < .001; OR: 2.97; 95% CI: 1.63-5.43; < .001).
In this high-fidelity group of patients with SAE, continuous, NIRS-based monitoring can identify blood pressure ranges that improve autoregulation. This is important given the association between cerebral autoregulatory function and severity of encephalopathy. Individualizing blood pressure goals using bedside autoregulation monitoring may better preserve cerebral perfusion in SAE than current practice.
脑自动调节功能受损和脑灌注不足可能在脓毒症相关性脑病(SAE)患者的高发病率和高死亡率中起关键作用。床边脑自动调节功能评估可能有助于个体化血流动力学目标,从而优化脑灌注。我们假设近红外光谱(NIRS)衍生的脑血氧饱和度测定法可以识别出能增强SAE患者自动调节功能的血压范围,并且自动调节功能紊乱与脑病严重程度相关。
对直接由脓毒症引起的急性脑病成年患者,使用基于NIRS的多模式监测连续随访12小时。我们利用局部脑血氧饱和度与平均动脉压(MAP)之间的时间相关性来确定脑血氧饱和度指数(COx),作为脑自动调节功能的一项指标。为每位患者构建自动调节曲线,将平均COx值按MAP在3个连续的4小时时间段内进行排序;在每个时间段内确定最佳压力(MAP),即与最稳健自动调节功能(最低COx)相关的MAP。用格拉斯哥昏迷量表(GCS)评估脑病严重程度。
6例符合严格标准的颅外脓毒症患者纳入研究,这些标准包括未使用药物镇静且无神经疾病病史。所有患者均确定了最佳MAP,范围为55至115 mmHg。此外,在监测期间,个体患者的MAP随时间变化。基于COx的自动调节功能紊乱与较差的神经状态(GCS < 13)相关,无论是否控制年龄和脓毒症严重程度(校正比值比[OR]:2.11;95%置信区间[CI]:1.77 - 2.52;P <.001;OR:2.97;95% CI:1.63 - 5.43;P <.001)。
在这组高保真的SAE患者中,基于NIRS的连续监测可以识别出能改善自动调节功能的血压范围。鉴于脑自动调节功能与脑病严重程度之间的关联,这一点很重要。与当前做法相比,使用床边自动调节功能监测来个体化血压目标可能能更好地维持SAE患者的脑灌注。