Nishikido Toshiyuki, Ray Kausik K
Imperial Centre for Cardiovascular Disease Prevention, Department of Primary Care and Public Health, School of Public Health, Imperial College London, London, United Kingdom.
Department of Cardiovascular medicine, Saga University, Saga, Japan.
Front Cardiovasc Med. 2019 Jan 29;5:199. doi: 10.3389/fcvm.2018.00199. eCollection 2018.
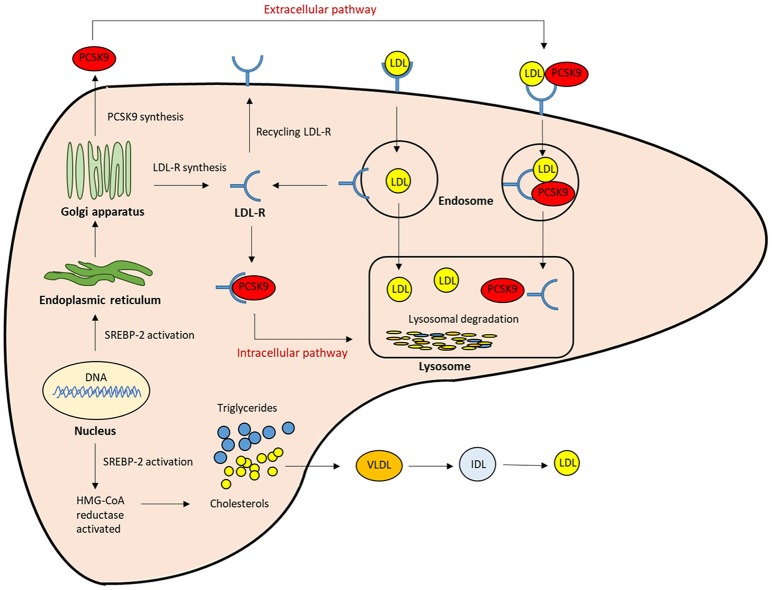
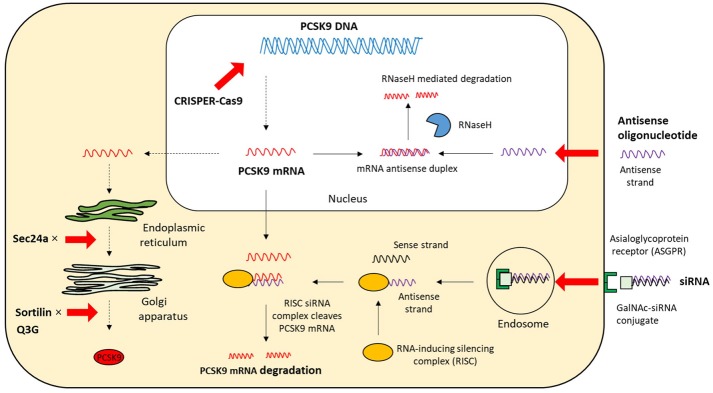
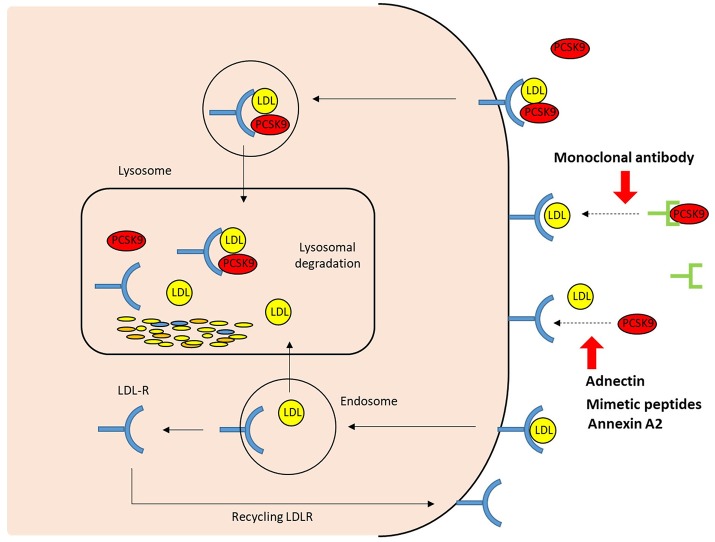
Low-density lipoprotein (LDL) is one of the principal risk factors for atherosclerosis. Circulating LDL particles can penetrate into the sub-endothelial space of arterial walls. These particles undergo oxidation and promote an inflammatory response, resulting in injury to the vascular endothelial wall. Persistent elevation of LDL-cholesterol (LDL-C) is linked to the progression of fatty streaks to lipid-rich plaque and thus atherosclerosis. LDL-C is a causal factor for atherosclerotic cardiovascular disease and lowering it is beneficial across a range of conditions associated with high risk of cardiovascular events. Therefore, all guidelines-recommended initiations of statin therapy for patients at high cardiovascular risk is irrespective of LDL-C. In addition, intensive LDL-C lowering therapy with statins has been demonstrated to result in a greater reduction of cardiovascular event risk in large clinical trials. However, many high-risk patients receiving statins fail to achieve the guideline-recommended reduction in LDL-C levels in routine clinical practice. Moreover, low levels of adherence and often high rates of discontinuation demand the need for further therapies. Ezetimibe has typically been used as a complement to statins when further LDL-C reduction is required. More recently, proprotein convertase subtilisin kexin 9 (PCSK9) has emerged as a novel therapeutic target for lowering LDL-C levels, with PCSK9 inhibitors offering greater reductions than feasible through the addition of ezetimibe. PCSK9 monoclonal antibodies have been shown to not only considerably lower LDL-C levels but also cardiovascular events. However, PCSK9 monoclonal antibodies require once- or twice-monthly subcutaneous injections. Further, their manufacturing process is expensive, increasing the cost of therapy. Therefore, several non-antibody treatments to inhibit PCSK9 function are being developed as alternative approaches to monoclonal antibodies. These include gene-silencing or editing technologies, such as antisense oligonucleotides, small interfering RNA, and the clustered regularly interspaced short palindromic repeats/Cas9 platform; small-molecule inhibitors; mimetic peptides; adnectins; and vaccination. In this review, we summarize the current knowledge base on the role of PCSK9 in lipid metabolism and an overview of non-antibody approaches for PCSK9 inhibition and their limitations. The subsequent development of alternative approaches to PCSK9 inhibition may give us more affordable and convenient therapeutic options for the management of high-risk patients.
低密度脂蛋白(LDL)是动脉粥样硬化的主要危险因素之一。循环中的LDL颗粒可穿透动脉壁的内皮下间隙。这些颗粒发生氧化并引发炎症反应,导致血管内皮壁损伤。LDL胆固醇(LDL-C)持续升高与脂肪条纹发展为富含脂质的斑块以及动脉粥样硬化相关。LDL-C是动脉粥样硬化性心血管疾病的一个致病因素,降低LDL-C对一系列心血管事件高风险相关病症有益。因此,所有指南推荐对心血管高风险患者启动他汀类药物治疗时不考虑LDL-C水平。此外,在大型临床试验中已证明,强化他汀类药物降低LDL-C治疗可更大程度降低心血管事件风险。然而,在常规临床实践中,许多接受他汀类药物治疗的高风险患者未能达到指南推荐的LDL-C水平降低幅度。此外,依从性低且停药率往往较高,这就需要进一步的治疗方法。当需要进一步降低LDL-C时,依折麦布通常用作他汀类药物的补充药物。最近,前蛋白转化酶枯草溶菌素9(PCSK9)已成为降低LDL-C水平的一个新治疗靶点,PCSK9抑制剂比添加依折麦布能更大程度地降低LDL-C。已证明PCSK9单克隆抗体不仅能大幅降低LDL-C水平,还能降低心血管事件。然而,PCSK9单克隆抗体需要每月皮下注射一次或两次。此外,其生产过程昂贵,增加了治疗成本。因此,正在开发几种抑制PCSK9功能的非抗体治疗方法作为单克隆抗体的替代方法。这些方法包括基因沉默或编辑技术,如反义寡核苷酸、小干扰RNA和成簇规律间隔短回文重复序列/Cas9平台;小分子抑制剂;模拟肽;adnectin;以及疫苗接种。在本综述中,我们总结了关于PCSK9在脂质代谢中作用的现有知识库,以及PCSK9抑制的非抗体方法及其局限性的概述。PCSK9抑制替代方法的后续发展可能会为高危患者的管理提供更经济实惠且方便的治疗选择。