Liver Imaging Group, Department of Radiology, University of California San Diego, San Diego, CA, USA.
School of Medicine, University of California San Diego, San Diego, CA, USA.
Eur Radiol. 2019 Sep;29(9):5073-5081. doi: 10.1007/s00330-019-06058-2. Epub 2019 Feb 26.
This study assesses the risk of progression of Liver Imaging Reporting and Data System (LI-RADS) categories, and the effects of inter-exam changes in modality or radiologist on LI-RADS categorization.
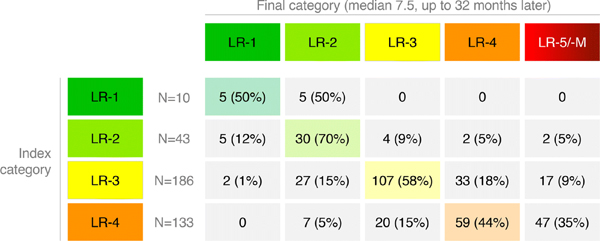
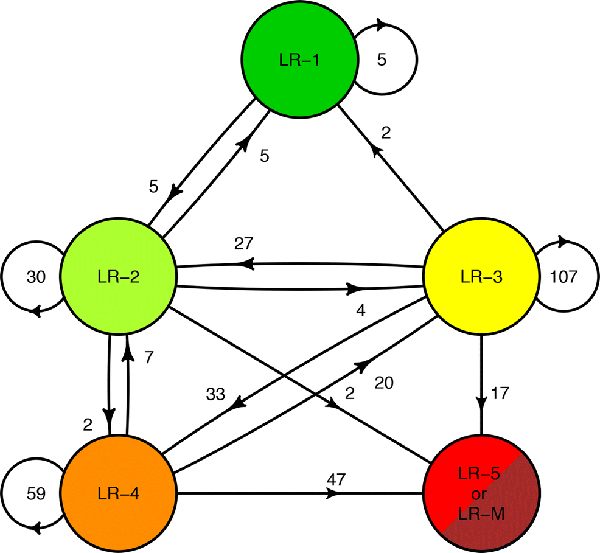
Clinical LI-RADS v2014 CT and MRI exams at our institution between January 2014 and September 2017 were retrospectively identified. Untreated LR-1, LR-2, LR-3, and LR-4 observations with at least one follow-up exam were included. Three hundred and seventy-two observations in 214 patients (149 male, 65 female, mean age 61 ± 10 years) were included during the study period (715 exams total). Cumulative incidence curves for progression to malignant LI-RADS categories (LR-5 or LR-M) and to LR-4 or higher were generated for each index category and compared using log-rank tests with a resampling extension. Relationships between inter-exam changes in LI-RADS category and modality or radiologist, adjusted for inter-exam time intervals, were modeled using mixed effect logistic regressions.
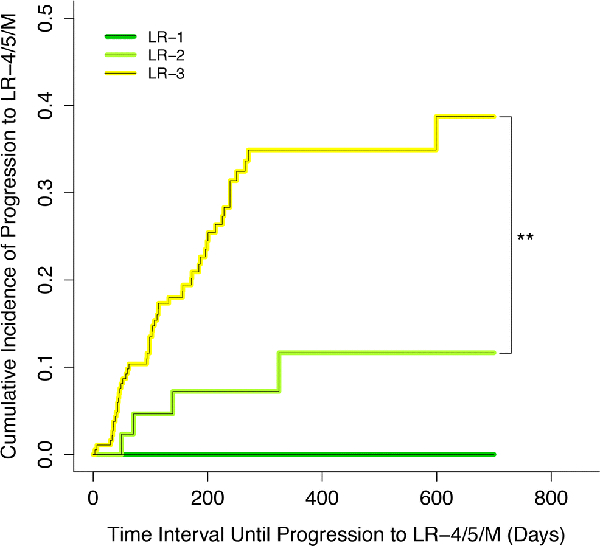
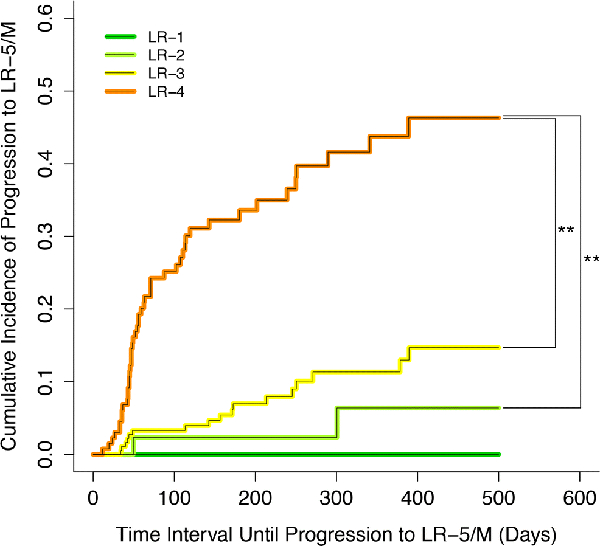
Median inter-exam follow-up interval and total follow-up duration were 123 and 227 days, respectively. Index LR-1, LR-2, LR-3, and LR-4 differed significantly in their cumulative incidences of progression to malignant categories (p < 0.0001), which were 0%, 2%, 7%, and 32% at 6 months, respectively. Index LR-1, LR-2, and LR-3 differed significantly in cumulative incidences of progression to LR-4 or higher (p = 0.003). MRI-MRI exam pairs had more stable LI-RADS categorization compared to CT-CT (OR = 0.460, p = 0.0018).
LI-RADS observations demonstrate increasing risk of progression to malignancy with increasing category ranging from 0% for LR-1 to 32% for LR-4 at 6 months. Inter-exam modality changes are associated with LI-RADS category changes.
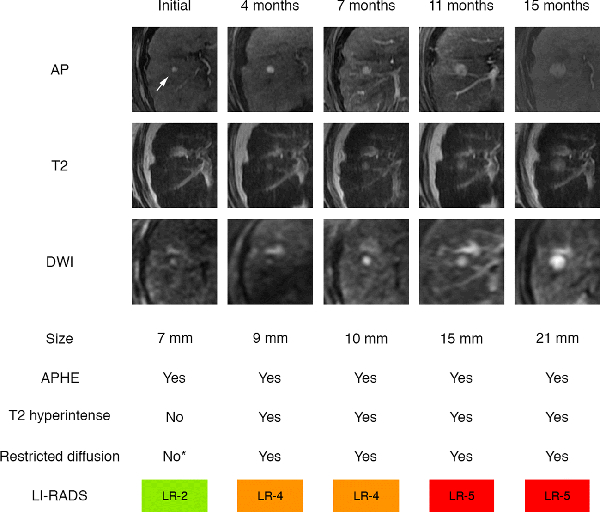
• While the majority of LR-2 observations remain stable over long-term follow-up, LR-3 and especially LR-4 observations have a higher risk for category progression. • Category transitions between sequential exams using different modalities (CT vs. MRI) may reflect modality differences rather than biological change. MRI, especially with the same type of contrast agent, may provide the most reproducible categorization, although this needs additional validation. • In a clinical practice setting, in which radiologists refer to prior imaging and reports, there was no significant association between changes in radiologist and changes in LI-RADS categorization.
本研究评估了肝脏成像报告和数据系统(LI-RADS)分类的进展风险,以及检查方式或放射科医生改变对 LI-RADS 分类的影响。
回顾性分析了我院 2014 年 1 月至 2017 年 9 月期间的临床 LI-RADS v2014 CT 和 MRI 检查。纳入至少有一次随访检查的未经治疗的 LR-1、LR-2、LR-3 和 LR-4 观察。在研究期间,共纳入了 214 例患者的 372 个观察(149 例男性,65 例女性,平均年龄 61±10 岁)(共 715 次检查)。为每个指数类别生成进展为恶性 LI-RADS 类别(LR-5 或 LR-M)和进展为 LR-4 或更高的累积发生率曲线,并使用对数秩检验和重采样扩展进行比较。使用混合效应逻辑回归模型,对检查方式或放射科医生改变与 LI-RADS 类别的关系进行建模,同时调整了检查间隔时间。
中位随访间隔和总随访时间分别为 123 天和 227 天。指数 LR-1、LR-2、LR-3 和 LR-4 的恶性分类进展累积发生率差异具有统计学意义(p<0.0001),分别为 0%、2%、7%和 32%,在 6 个月时。指数 LR-1、LR-2 和 LR-3 的进展为 LR-4 或更高的累积发生率差异具有统计学意义(p=0.003)。与 CT-CT 相比,MRI-MRI 检查对的 LI-RADS 分类更稳定(OR=0.460,p=0.0018)。
LI-RADS 观察结果表明,随着分类的增加,恶性进展的风险逐渐增加,从 LR-1 的 0%到 LR-4 的 32%,在 6 个月时。检查方式的改变与 LI-RADS 分类的改变有关。
虽然大多数 LR-2 观察结果在长期随访中保持稳定,但 LR-3 尤其是 LR-4 观察结果的分类进展风险更高。
使用不同方式(CT 与 MRI)进行连续检查时的类别转换可能反映了方式的差异,而不是生物学的变化。MRI,特别是使用相同类型的造影剂,可能提供最具可重复性的分类,但这需要进一步验证。
在临床实践中,放射科医生会参考先前的影像学和报告,放射科医生的改变与 LI-RADS 分类的改变之间没有显著关联。