Kuwornu John Paul, Teare Gary F, Quail Jacqueline M, Forget Evelyn, Muthukumarana Saman, Wang Xiaoyun E, Osman Meric, Lix Lisa M
Department of Community Health Sciences, University of Manitoba, Winnipeg, MB, Canada.
Saskatchewan Health Quality Council, 111 Research Drive, Saskatoon, SK, Canada.
Can J Respir Ther. 2017 Summer;53(3):37-44. Epub 2017 Aug 1.
COPD is a high-cost disease and results in frequent contacts with the healthcare system. The study objective was to compare the accuracy of classification models with different covariates for classifying COPD patients into cost groups.
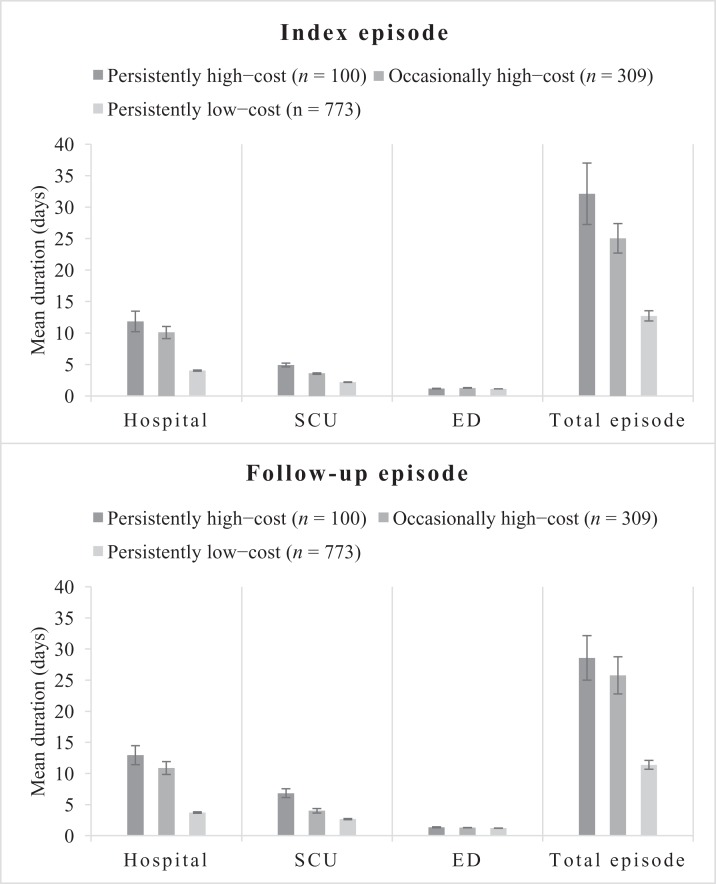
Linked health administrative databases from Saskatchewan, Canada, were used to identify a cohort of newly diagnosed COPD patients (April 1, 2007 to March 31, 2011) and their episodes of healthcare encounters for disease exacerbations. Total costs of the first and follow-up episodes were computed and patients were categorized as persistently high cost, occasionally high cost, and persistently low cost based on cumulative cost distribution ranking using the 75th percentile cutoff for high-cost status. Classification accuracy was compared for seven multinomial logistic regression models containing socio-demographic characteristics (i.e., base model), and socio-demographic and prior healthcare use characteristics (i.e., comparator models).
Of the 1182 patients identified, 8.5% were classified as persistently high cost, 26.1% as occasionally high cost, and the remainder as persistently low cost. The persistently high-cost and occasionally high-cost patients incurred 10 times ($12 449 vs $1263) and seven times ($9334 vs $1263) more costs in their first exacerbation episode than persistently low-cost patients, respectively. Classification accuracy was 0.67 for the base model, whereas the comparator model containing socio-demographic and number of prior hospital admissions had the highest accuracy (0.72).
Costs associated with COPD exacerbation episodes are substantial. Adding prior hospitalization to socio-demographic characteristics produced the highest improvements in classification accuracy. Accurate classification models are important for identifying potential healthcare cost management strategies.
慢性阻塞性肺疾病(COPD)是一种高成本疾病,导致患者频繁与医疗保健系统接触。本研究的目的是比较使用不同协变量的分类模型将COPD患者分类到成本组中的准确性。
利用加拿大萨斯喀彻温省的联合卫生行政数据库,确定一组新诊断的COPD患者(2007年4月1日至2011年3月31日)及其疾病加重的医疗接触事件。计算首次和后续事件的总成本,并根据使用第75百分位数作为高成本状态临界值的累积成本分布排名,将患者分为持续高成本、偶尔高成本和持续低成本三类。比较了包含社会人口学特征(即基础模型)以及社会人口学和既往医疗使用特征(即比较模型)的七个多项逻辑回归模型的分类准确性。
在识别出的1182名患者中,8.5%被分类为持续高成本,26.1%为偶尔高成本,其余为持续低成本。在首次加重事件中,持续高成本和偶尔高成本患者分别比持续低成本患者多产生10倍(12449美元对1263美元)和7倍(9334美元对1263美元)的成本。基础模型的分类准确性为0.67,而包含社会人口学特征和既往住院次数的比较模型具有最高的准确性(0.72)。
与COPD加重事件相关的成本很高。在社会人口学特征中加入既往住院史可使分类准确性得到最大程度的提高。准确的分类模型对于确定潜在的医疗成本管理策略很重要。