Sawhney J P S, Mullasari Ajit, Kahali Dhiman, Mehta Vimal, Nair Tiny, Kaul Upendra, Hirematth M S
Sir Ganga Ram Hospital, Delhi, India.
Madras Medical Mission, Chennai, India.
Indian Heart J. 2019 Jan-Feb;71(1):25-31. doi: 10.1016/j.ihj.2018.12.005. Epub 2019 Jan 3.
Acute coronary syndrome (ACS) is associated with emergency hospitalizations, and there are limited real-world data on clinical outcomes in post-ACS Asian patients. This article presents data on the Indian subgroup from the Long-term Follow-up of Antithrombotic Management Patterns in Acute Coronary Syndrome Patients in Asia (EPICOR-Asia) study.
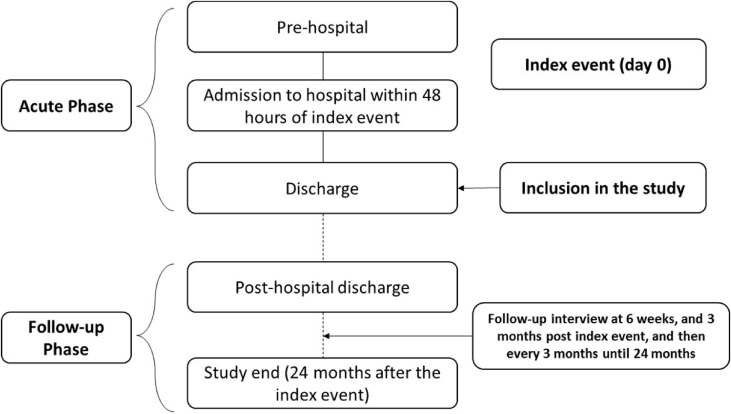
EPICOR included patients with ACS [ST-segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI), or unstable angina (UA)]. The study had two phases: acute phase and follow-up phase. The primary objective was to describe short- and long-term antithrombotic management patterns.
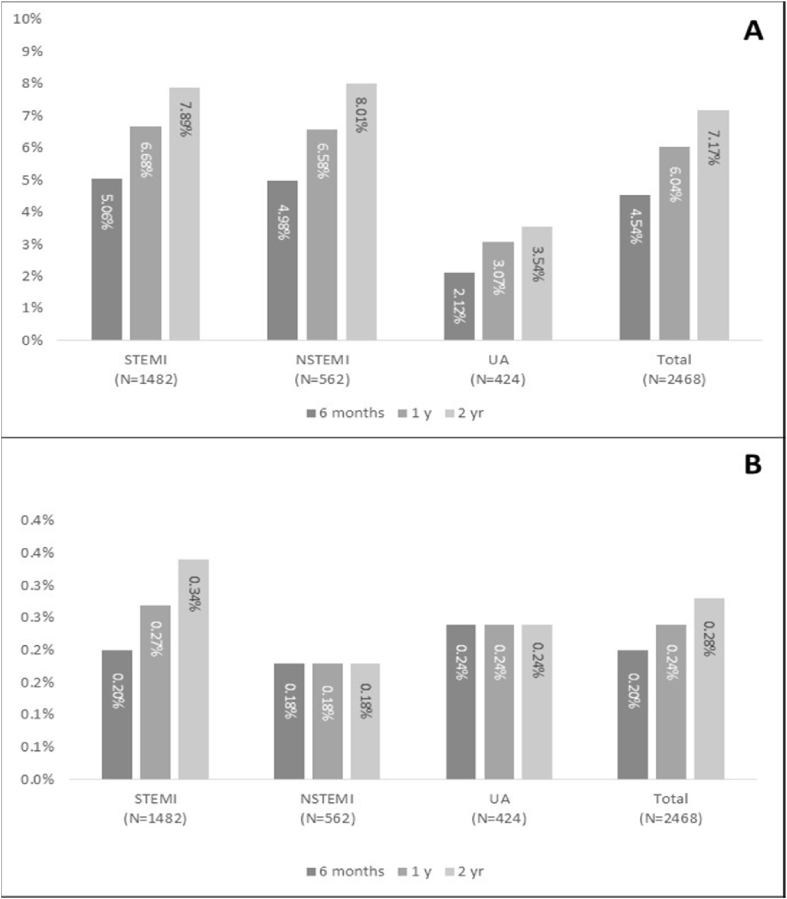
EPICOR-India enrolled 2468 patients (STEMI-1482; NSTEMI-562; and UA-424). Cardiovascular risk factors were present in 1362 (55.2%) patients. Prehospital care was received by 879 (35.6%) patients, and the median time from the symptom onset to the first medical attention was 3 h (0.08, 100.33). The most common drug regimen prescribed during the acute phase was ≥2 antiplatelet agents + anticoagulants with no glycoprotein IIb/IIIa inhibitors and at discharge were aspirin + clopidogrel. About 78.8% of patients were discharged on dual antiplatelet therapy (DAPT) and 16%, on single antiplatelet therapy (SAPT). At 23 months after discharge, 55.6% were on DAPT, while 16.4% were on SAPT. Postdischarge outcomes at 2 years included death in 165 (6.7%) patients, composite events of death, myocardial infarction (MI), or ischemic stroke in 182 (7.4%) patients, and bleeding events in seven (0.3%) patients.
This study showed a gap between international recommendations and implementation for managing ACS in Indian patients. Most of the patients prefer to undergo invasive management instead of non-invasive therapy. At the end of the 2-year follow-up, more than half of the population was receiving DAPT, with most patients on receiving a combination of aspirin and clopidogrel. The mortality along with composite events of death, MI, or ischemic stroke was highest for patients with NSTEMI.
急性冠状动脉综合征(ACS)与紧急住院治疗相关,而关于亚洲ACS后患者临床结局的真实世界数据有限。本文展示了亚洲急性冠状动脉综合征患者抗栓治疗管理模式长期随访研究(EPICOR-Asia)中印度亚组的数据。
EPICOR纳入了ACS患者[ST段抬高型心肌梗死(STEMI)、非ST段抬高型心肌梗死(NSTEMI)或不稳定型心绞痛(UA)]。该研究有两个阶段:急性期和随访期。主要目标是描述短期和长期抗栓治疗管理模式。
EPICOR-印度纳入了2468例患者(STEMI-1482例;NSTEMI-562例;UA-424例)。1362例(55.2%)患者存在心血管危险因素。879例(35.6%)患者接受了院前治疗,从症状发作到首次就医的中位时间为3小时(0.08,100.33)。急性期最常用的药物治疗方案是≥2种抗血小板药物+抗凝药物,不使用糖蛋白IIb/IIIa抑制剂,出院时为阿司匹林+氯吡格雷。约78.8%的患者出院时接受双联抗血小板治疗(DAPT),16%接受单联抗血小板治疗(SAPT)。出院23个月时,55.6%的患者接受DAPT,而16.4%的患者接受SAPT。2年的出院后结局包括165例(6.7%)患者死亡,182例(7.4%)患者发生死亡、心肌梗死(MI)或缺血性卒中的复合事件,7例(0.3%)患者发生出血事件。
本研究显示了印度患者ACS管理的国际推荐与实施之间存在差距。大多数患者倾向于接受侵入性治疗而非非侵入性治疗。在2年随访结束时,超过一半的人群接受DAPT,大多数患者接受阿司匹林和氯吡格雷联合治疗。NSTEMI患者的死亡率以及死亡、MI或缺血性卒中的复合事件最高。