Division of Cardiovascular and Thoracic Surgery, Department of Surgery, Duke University Medical Center, Durham, North Carolina.
Division of Cardiovascular and Thoracic Surgery, Department of Surgery, Duke University Medical Center, Durham, North Carolina.
Ann Thorac Surg. 2019 Aug;108(2):377-383. doi: 10.1016/j.athoracsur.2019.03.053. Epub 2019 Apr 18.
Current guidelines do not routinely recommend adjuvant therapy for resected stage I large cell lung neuroendocrine cancer (LCNEC). However, data regarding the role of adjuvant therapy in early LCNEC are limited. This National Cancer Database (NCDB) analysis was performed to improve the evidence guiding adjuvant therapy for early LCNEC.
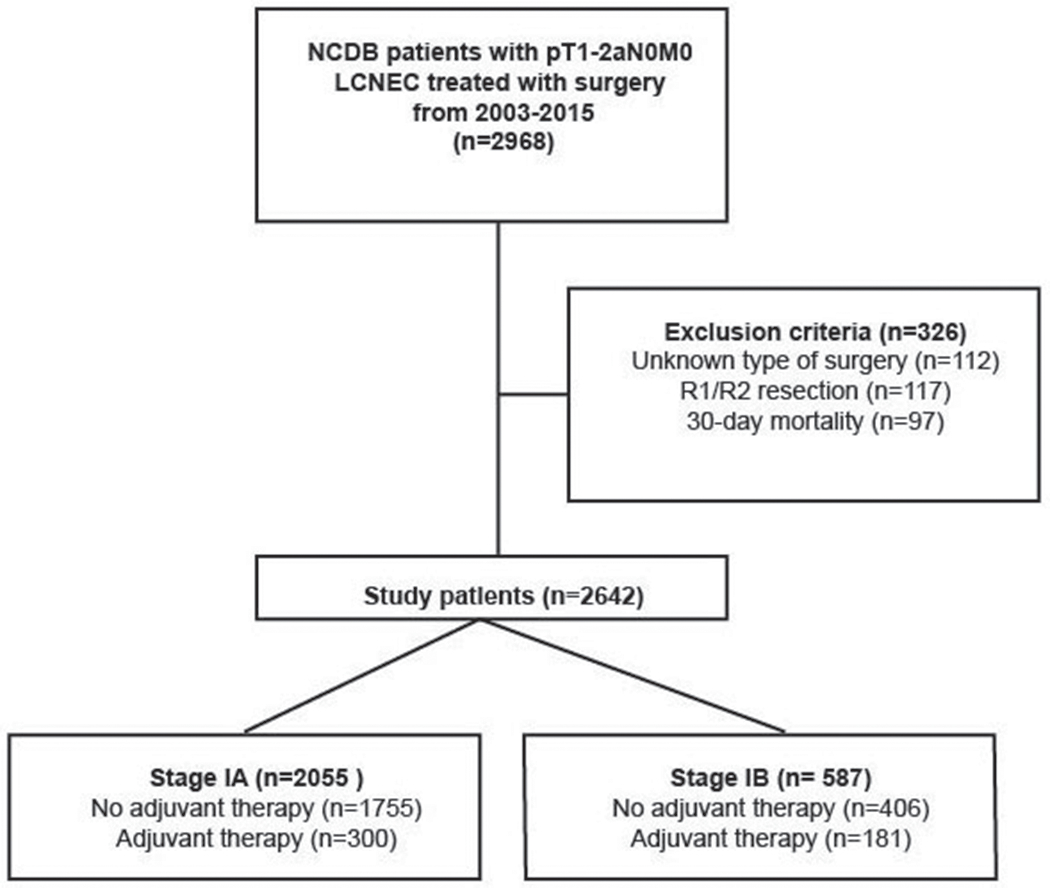
Overall survival (OS) of patients with pathologic T1-2a N0 M0 LCNEC who underwent resection in the NCDB from 2003 to 2015 was evaluated with Kaplan-Meier and multivariable Cox proportional hazards analyses. Patients who died within 30 days of surgery and with more than R0 resection were excluded.
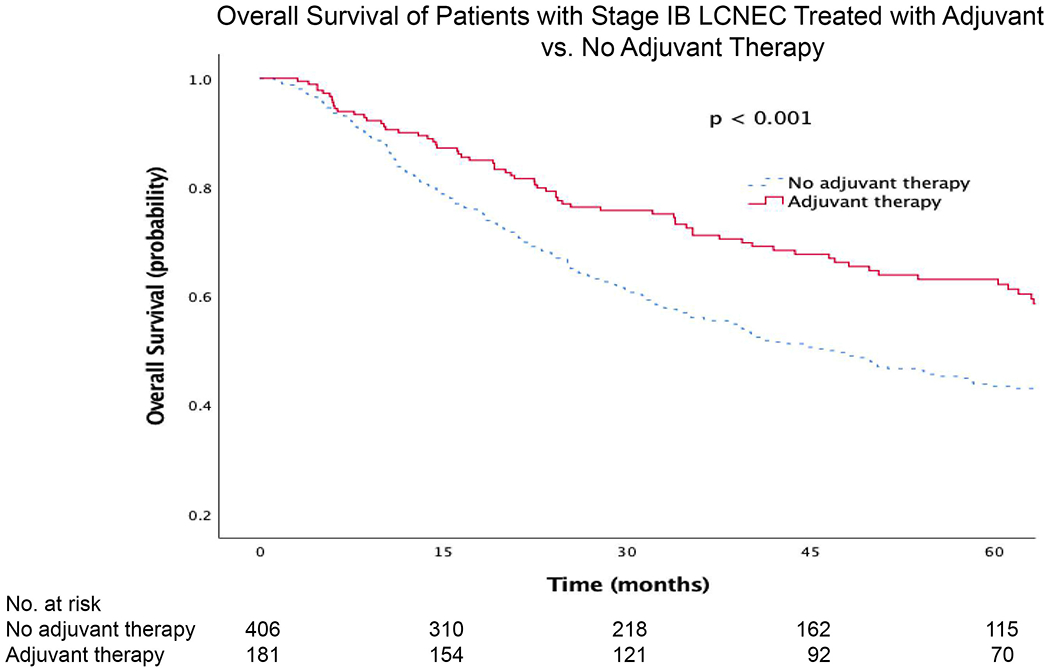
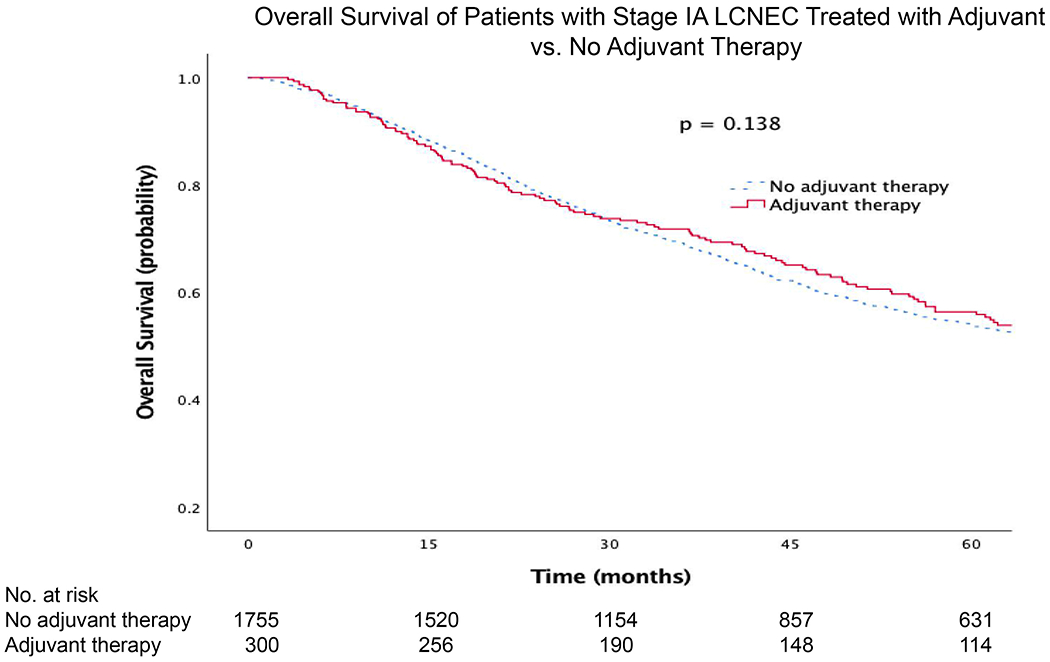
Of 2642 patients meeting study criteria, 481 (18%) received adjuvant therapy. Adjuvant chemotherapy in stage IB patients was associated with a significant increase in OS (hazard ratio, 0.67; 95% confidence interval, 0.50 to 0.90). However, there was no significant difference in survival between adjuvant chemotherapy and no adjuvant therapy for stage IA LCNEC (hazard ratio, 0.92; 95% confidence interval, 0.75 to 1.11). Adjuvant radiotherapy, whether alone or combined with chemotherapy, was not associated with a change in OS. In subgroup analysis, patients receiving adjuvant chemotherapy after lobar resection for stage IB LCNEC had a significant survival benefit compared with patients not receiving adjuvant therapy.
In early-stage LCNEC, adjuvant chemotherapy appears to confer an additional overall survival advantage only in patients with completely resected stage IB LCNEC and not for patients with completely resected stage IA LCNEC.
目前的指南并未常规推荐对接受手术切除的 I 期大细胞神经内分泌肺癌(LCNEC)患者进行辅助治疗。然而,有关早期 LCNEC 辅助治疗作用的数据有限。本项国家癌症数据库(NCDB)分析旨在为指导早期 LCNEC 辅助治疗提供更多证据。
采用 Kaplan-Meier 法和多变量 Cox 比例风险分析评估了 2003 年至 2015 年期间在 NCDB 中接受手术切除且病理分期为 T1-2aN0M0 LCNEC 的患者的总生存期(OS)。排除术后 30 天内死亡且 R0 切除不完全的患者。
在符合研究标准的 2642 例患者中,有 481 例(18%)接受了辅助治疗。IB 期患者接受辅助化疗可显著提高 OS(风险比,0.67;95%置信区间,0.50 至 0.90)。然而,IA 期 LCNEC 患者接受辅助化疗与不接受辅助化疗之间的生存无显著差异(风险比,0.92;95%置信区间,0.75 至 1.11)。单独或联合使用化疗的辅助放疗与 OS 无变化相关。亚组分析显示,IB 期 LCNEC 行肺叶切除术后接受辅助化疗的患者与未接受辅助化疗的患者相比,生存获益显著。
在早期 LCNEC 中,辅助化疗似乎仅在完全切除的 IB 期 LCNEC 患者中提供了额外的总体生存优势,而在完全切除的 IA 期 LCNEC 患者中则没有。