Department of Psychiatry, School of Medicine, Yale University.
J Consult Clin Psychol. 2019 Jun;87(6):530-540. doi: 10.1037/ccp0000404. Epub 2019 Apr 22.
To examine whether race predicted or moderated response to treatments for binge-eating disorder (BED).
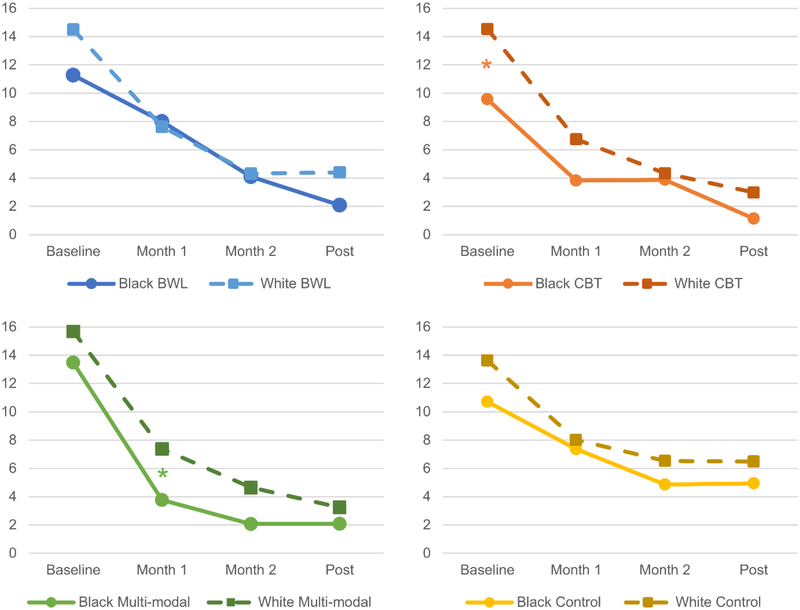
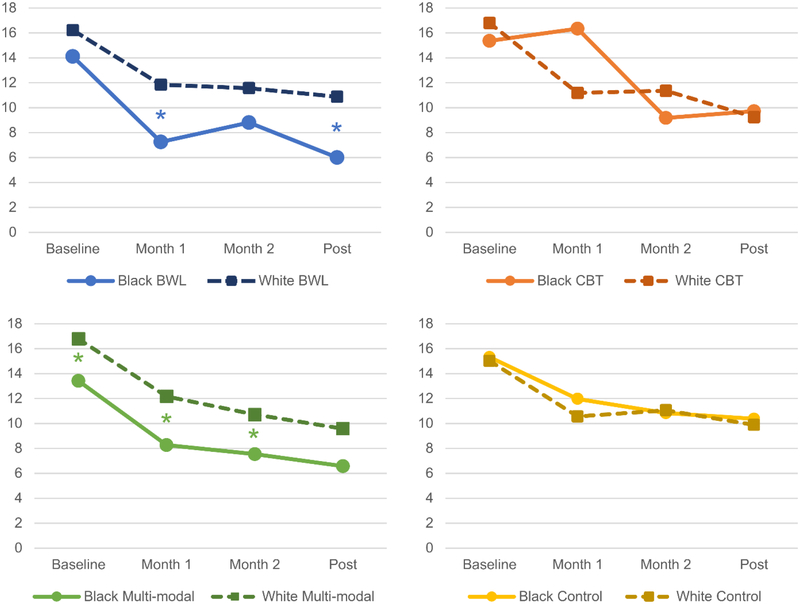
Participants were 592 adults (n = 113 Black; n = 479 White) with DSM-IV-defined BED who participated in randomized controlled trials (RCTs) at 1 medical center. Data were aggregated from RCTs for BED testing cognitive-behavioral therapy, behavioral weight loss, multimodal treatment, and/or control conditions. Participants had weight and height measured and were assessed using established interviews and self-report measures at baseline, throughout treatment, and post treatment.
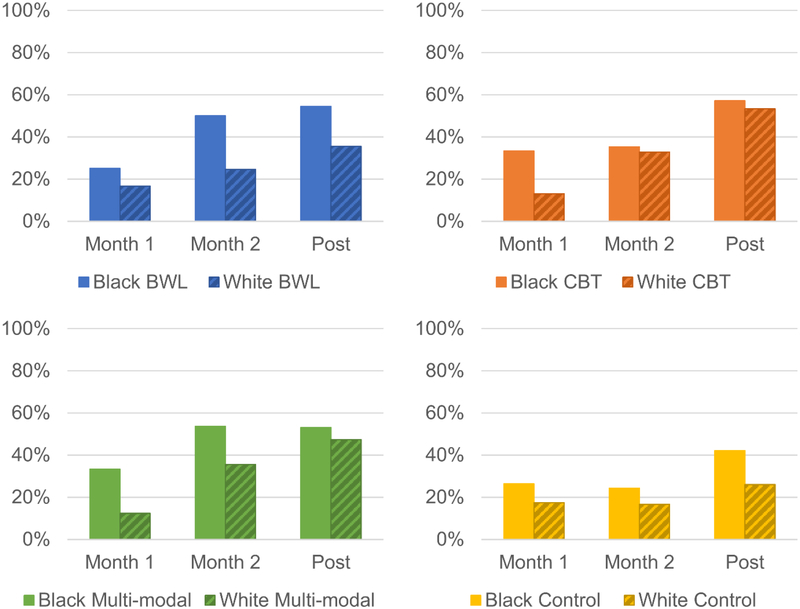
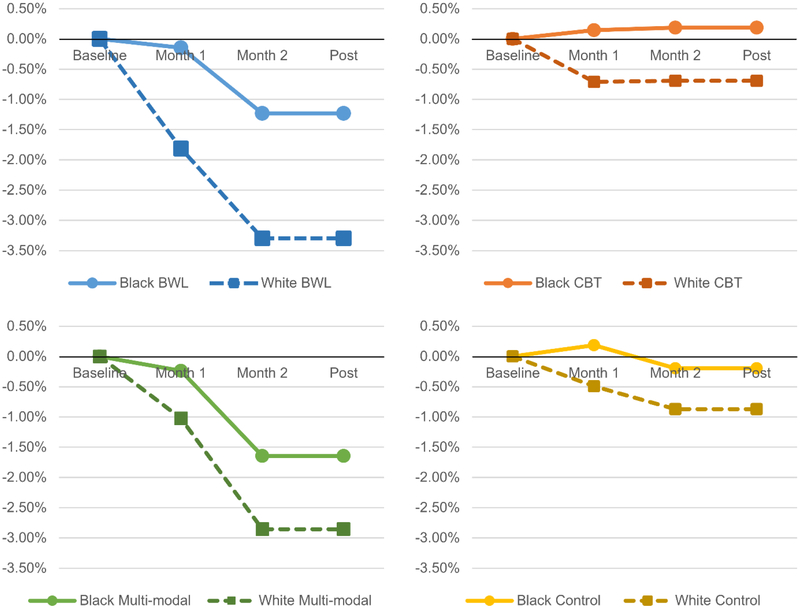
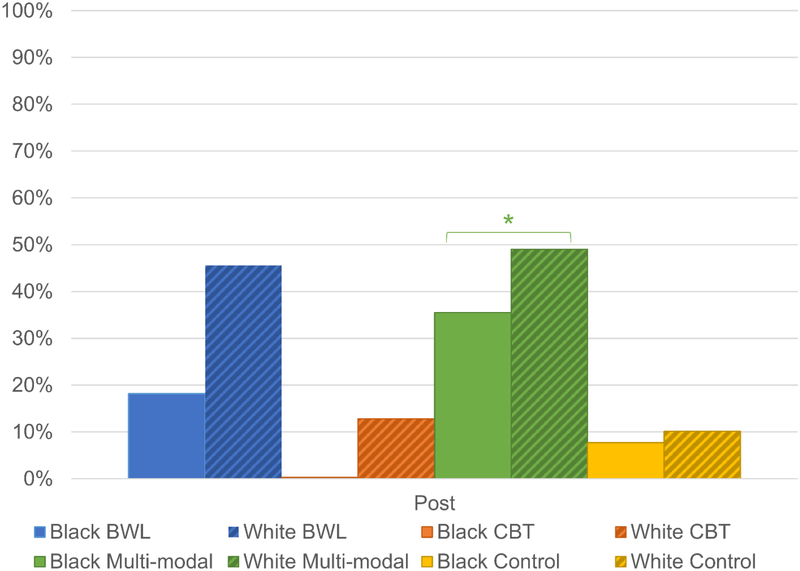
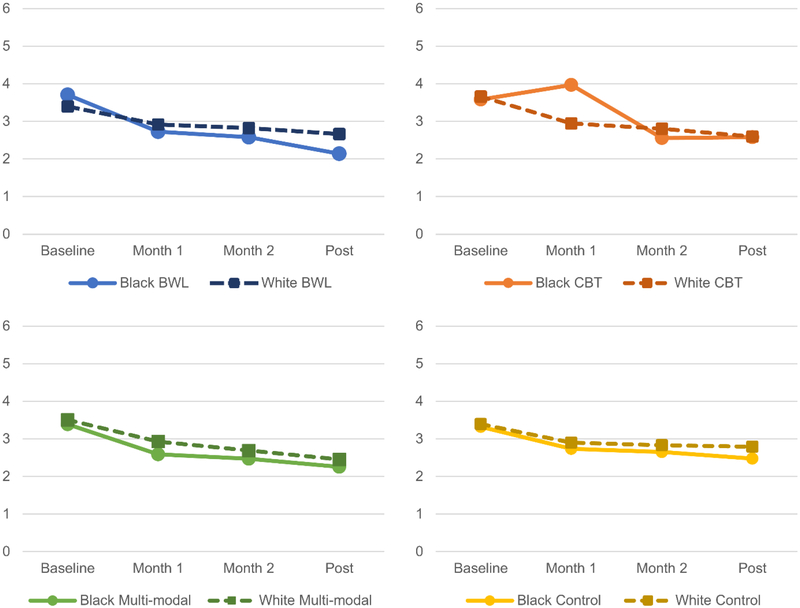
Race did not significantly moderate treatment outcomes. Mixed models revealed a main effect of race: Black participants had fewer binge-eating episodes and lower depression than White participants across time points. Race also had a main effect in generalized estimating equations with a significantly greater proportion of Black participants achieving binge-eating remission than White participants. Race did not predict percent weight loss, but a significantly lower proportion of Black participants attained 5% weight loss than White participants. Race did not significantly predict global eating-disorder severity.
Despite disparities in treatment-seeking reported in epidemiological and RCT studies, Black individuals appear to have comparable or better treatment outcomes in BED treatment research compared with White individuals, except they were less likely to attain 5% weight loss at post treatment. This suggests that disseminating evidence-based treatments for BED among diverse populations holds promise and treatments may not require further adaptation prior to dissemination. Implementation research is needed to test treatment effectiveness across diverse providers, settings, and patient groups to improve understanding of potential predictors and moderators. (PsycINFO Database Record (c) 2019 APA, all rights reserved).
探讨种族是否能预测或调节暴食障碍(BED)的治疗反应。
参与者为 592 名符合 DSM-IV 标准的 BED 成年人(n=113 名黑人;n=479 名白人),他们在 1 家医疗中心参加了随机对照试验(RCT)。从针对 BED 的 RCT 中汇总数据,测试认知行为疗法、行为减肥、多模式治疗和/或对照条件。参与者的体重和身高进行了测量,并在基线、治疗期间和治疗后使用既定的访谈和自我报告措施进行了评估。
种族并没有显著调节治疗结果。混合模型显示种族存在主要影响:与白人参与者相比,黑人参与者在各时间点的暴食发作次数更少,抑郁程度更低。种族在广义估计方程中也有主要影响,黑人参与者达到暴食缓解的比例显著高于白人参与者。种族并不预测体重减轻的百分比,但黑人参与者达到 5%体重减轻的比例明显低于白人参与者。种族并不显著预测整体饮食障碍严重程度。
尽管在流行病学和 RCT 研究中报告了治疗寻求方面的差异,但与白人参与者相比,黑人个体在 BED 治疗研究中似乎具有相当或更好的治疗结果,除了他们在治疗后达到 5%体重减轻的比例较低。这表明在不同人群中传播 BED 的基于证据的治疗方法有希望,并且在传播之前,治疗方法可能不需要进一步的调整。需要开展实施研究,以测试不同提供者、环境和患者群体中治疗的有效性,从而更好地了解潜在的预测因素和调节因素。(APA,2019,所有权利保留)。