Department of Radiology and Nuclear Medicine, University Medical Center Utrecht, Utrecht, the Netherlands.
Image Sciences Institute, University Medical Center Utrecht, Utrecht, the Netherlands.
Med Phys. 2019 Jul;46(7):3156-3164. doi: 10.1002/mp.13559. Epub 2019 May 27.
The limited axial coverage of many computed tomography (CT) scanners poses a high risk on false negative findings in cerebral CT-perfusion (CTP) imaging. Axial coverage may be increased by moving the table back and forth during image acquisition. However, this method often increases the acquisition interval between CT frames, which may influence the CTP analysis. In this study, we evaluated the influence of different acquisition intervals on quantitative perfusion maps and infarct volumes by analyzing patient data with three CTP analysis methods.
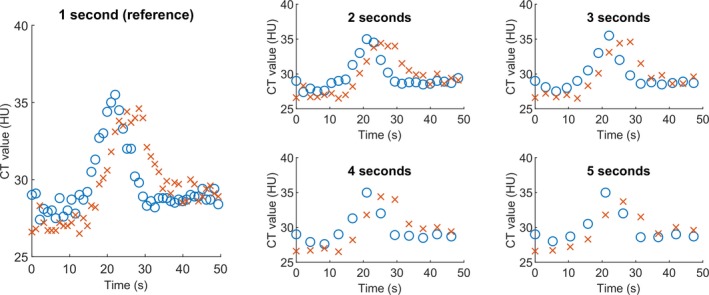
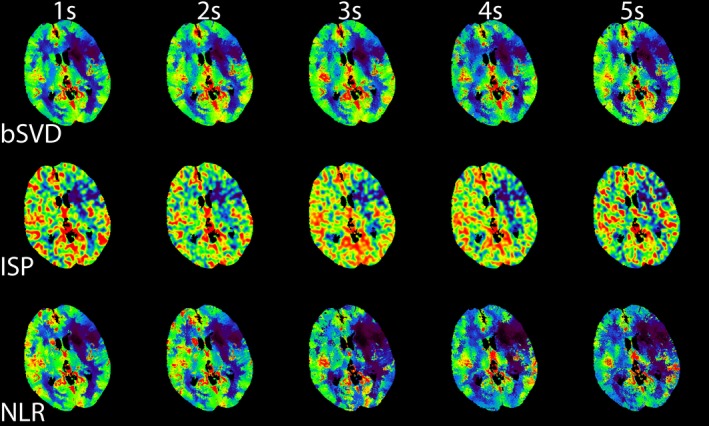
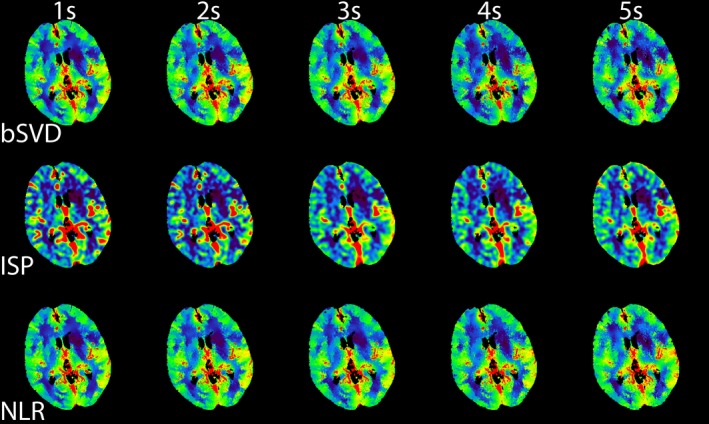
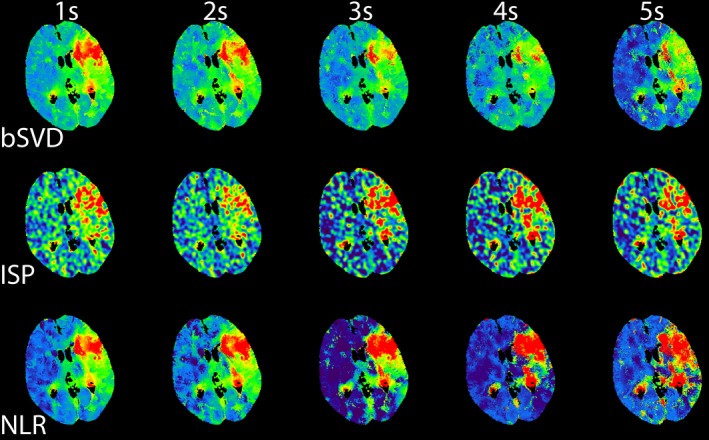
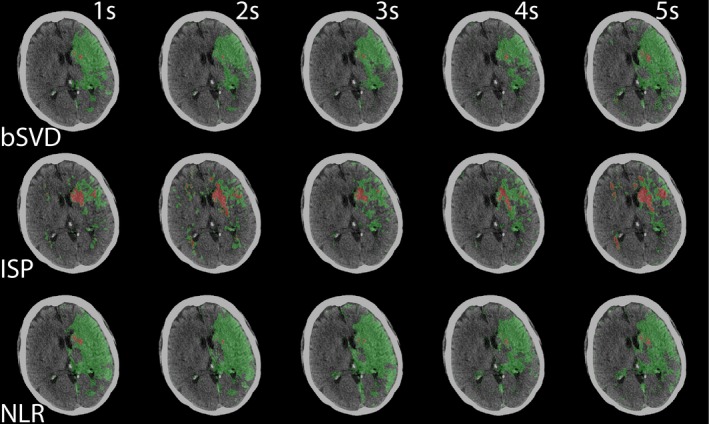
CT-perfusion data from 25 patients with ischemic stroke were used for this study. The acquisition interval was synthetically reduced from 1 to 5 s before calculating perfusion values, which included cerebral blood flow (CBF), cerebral blood volume (CBV), and mean transit time (MTT). The color scaling of the perfusion was scaled such that the mean perfusion value had the same color-coding as the mean perfusion in the 1 s reference. Also, infarct core and penumbra volumes (summary map) were calculated using default thresholds of CBV and relative MTT (rMTT). The original, 1 s acquisition interval scan served as the reference standard. A commercial block-circulant singular value decomposition (bSVD) based method (ISP; Philips Healthcare), a non-commercial bSVD method, and a non-linear regression (NLR) model-based method were evaluated.
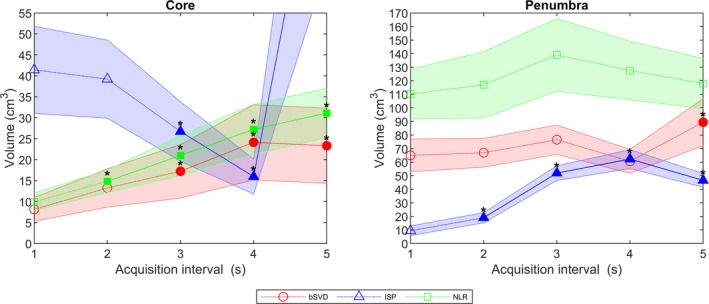
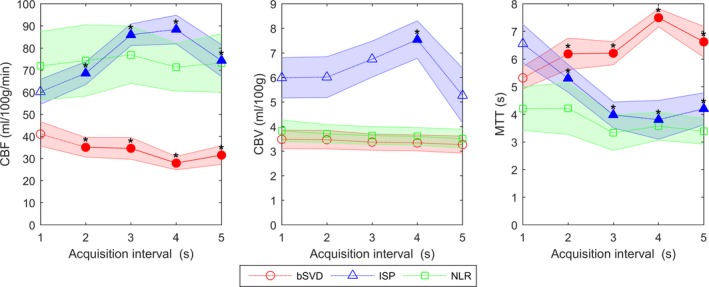
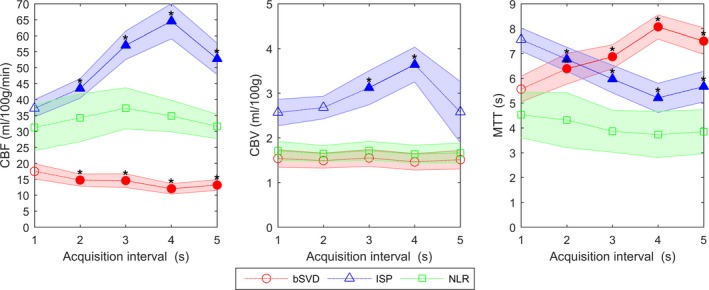
Cerebral blood volume values generated with bSVD and NLR were not significantly different from the reference standard, while ISP showed significant differences for acquisition intervals of 3 and 4 s. MTT and CBF values generated with bSVD and ISP were significantly different for all acquisition intervals, whereas NLR did not show any significant differences. Calibrated perfusion maps were able to distinguish healthy from infarcted tissue up to an acquisition interval of 5 s for all methods. The infarct core volumes were significantly different for acquisition intervals of 2 (NLR) and 3 s (bSVD and ISP) or greater. For the penumbra volumes, NLR showed no significant differences, while bSVD and ISP showed significant differences for the 5 s interval and for all intervals, respectively. Visual inspection of the summary maps indicated minor differences between the reference standard and acquisition intervals of 4 s or less (ISP) and 5 s or less (bSVD and NLR).
Altering the acquisition interval may introduce a bias in the perfusion parameters. Calibration of the visualization of the perfusion maps with increasing acquisition intervals allowed distinction between healthy and infarcted tissue. Infarct volumes based on relative MTT can be influenced by the acquisition interval, but visual inspection of the summary maps indicated minor differences between the reference standard and acquisition intervals up to 4 (ISP) and 5 s (bSVD and NLR). Taken together, axial coverage can be increased by prolonging the acquisition interval up to 5 s depending on the perfusion analysis.
许多计算机断层扫描(CT)扫描仪的轴向覆盖范围有限,这使得在脑 CT 灌注(CTP)成像中出现假阴性结果的风险很高。在图像采集过程中,可以通过前后移动工作台来增加轴向覆盖范围。然而,这种方法通常会增加 CT 帧之间的采集间隔,这可能会影响 CTP 分析。在这项研究中,我们通过分析三种 CTP 分析方法的患者数据,评估了不同采集间隔对定量灌注图和梗死体积的影响。
这项研究使用了 25 例缺血性脑卒中患者的 CTP 数据。在计算灌注值之前,综合将采集间隔从 1 秒缩短至 5 秒,灌注值包括脑血流量(CBF)、脑血容量(CBV)和平均通过时间(MTT)。灌注的颜色标度被缩放,使得平均灌注值的颜色编码与 1 秒参考值的平均灌注值的颜色编码相同。此外,还使用 CBV 和相对 MTT(rMTT)的默认阈值计算梗死核心和半影体积(摘要图)。原始的 1 秒采集间隔扫描作为参考标准。评估了一种基于商业循环奇异值分解(bSVD)的方法(ISP;飞利浦医疗保健公司)、一种非商业 bSVD 方法和一种基于非线性回归(NLR)模型的方法。
使用 bSVD 和 NLR 生成的 CBV 值与参考标准没有显著差异,而 ISP 则显示 3 秒和 4 秒采集间隔的差异显著。使用 bSVD 和 ISP 生成的 MTT 和 CBF 值在所有采集间隔都有显著差异,而 NLR 则没有显示任何显著差异。校准后的灌注图能够在所有方法中,直到采集间隔为 5 秒,区分健康组织和梗死组织。对于采集间隔为 2 秒(NLR)和 3 秒(bSVD 和 ISP)或更长时间的梗死核心体积,差异显著。对于半影体积,NLR 没有显示出显著差异,而 bSVD 和 ISP 则显示出 5 秒间隔和所有间隔的差异显著。对摘要图的直观检查表明,参考标准和采集间隔为 4 秒或更短(ISP)和 5 秒或更短(bSVD 和 NLR)之间存在微小差异。
改变采集间隔可能会对灌注参数产生偏差。通过增加采集间隔对灌注图的可视化进行校准,允许区分健康组织和梗死组织。基于相对 MTT 的梗死体积可能会受到采集间隔的影响,但对摘要图的直观检查表明,参考标准和采集间隔之间的差异较小,直到 4 秒(ISP)和 5 秒(bSVD 和 NLR)。总的来说,根据灌注分析,可以通过延长采集间隔来增加轴向覆盖范围,最长可达 5 秒。