Department of Surgery, Korea University Medical Center Ansan Hospital, Ansan, 15355, Korea.
Department of Breast and Endocrine Surgery, Hallym University Sacred Heart Hospital, Anyang, 14068, Korea.
World J Surg Oncol. 2019 Jun 13;17(1):101. doi: 10.1186/s12957-019-1645-1.
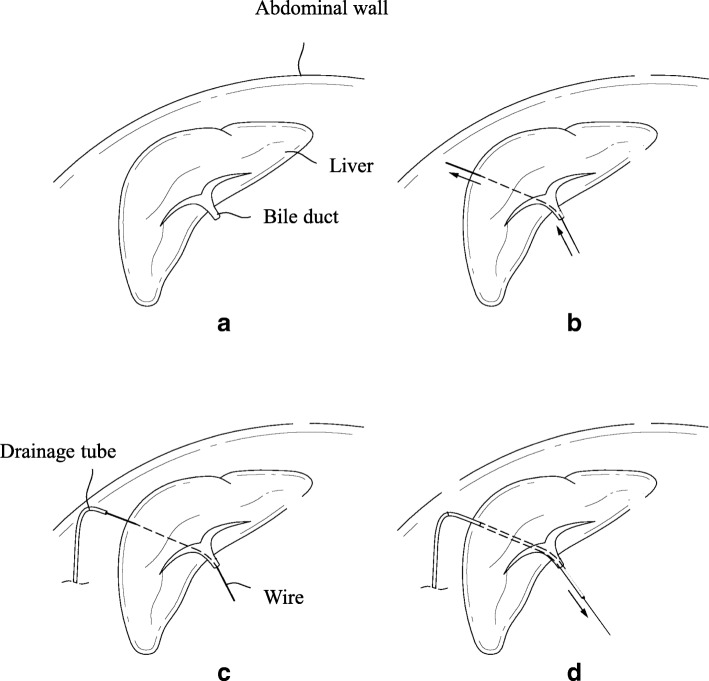
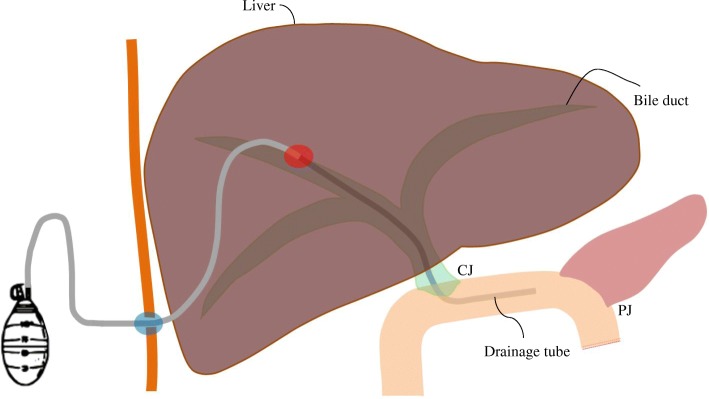
Leakage from the pancreatoenteric anastomosis has been one of the major complications of pancreaticoduodenectomy (PD). The aim of this study was to investigate the feasibility of retrograde installation of percutaneous transhepatic negative-pressure biliary drainage (RPTNBD), as part of which the drainage tube is intraoperatively inserted into the bile duct and afferent loop by surgical guidance to reduce pancreaticoenteric leakage after PD.
We retrospectively reviewed the medical records of the patients who underwent pylorus-preserving PD or Whipple's operation for a malignant disease between June 2012 and August 2016. We performed intraoperative RPTNBD to decompress the biliopancreatic limb in all patients and compared their clinical outcomes with those of internal controls.
Twenty-one patients were enrolled in this study. The operation time was 412.0 ± 92.8 min (range, 240-600 min). The duration of postoperative hospital stay was 39.4 ± 26.4 days (range, 13-105 days). Ten patients (47.6%) experienced morbidities of Clavien-Dindo grade > II, and 2 patients (9.5%) experienced pancreaticojejunostomy-related complications. The internal controls showed a higher incidence rate of pancreaticojejunostomy-related complications than the study participants (P = 0.020). Mortality occurred only in the internal controls.
For stabilizing the pancreaticoenteric anastomosis after PD for a malignant disease, RPTNBD is a feasible and effective procedure. When PD is combined with technically demanding procedures, including hepatectomy or vascular reconstruction, RPTNBD could prevent fulminant anastomotic failure.
胰肠吻合口漏是胰十二指肠切除术(PD)的主要并发症之一。本研究旨在探讨逆行经皮肝穿刺负压胆汁引流(RPTNBD)的可行性,术中通过手术引导将引流管插入胆管和输入襻,以降低 PD 后胰肠吻合口漏的风险。
我们回顾性分析了 2012 年 6 月至 2016 年 8 月期间因恶性疾病行保留幽门的 PD 或胰头十二指肠切除术的患者的病历。所有患者均在术中进行 RPTNBD 以减压胆胰肠袢,并将其临床结果与内部对照进行比较。
本研究共纳入 21 例患者。手术时间为 412.0±92.8 分钟(范围,240-600 分钟)。术后住院时间为 39.4±26.4 天(范围,13-105 天)。10 例患者(47.6%)发生 Clavien-Dindo 分级>Ⅱ级的并发症,2 例患者(9.5%)发生胰肠吻合口相关并发症。内部对照显示胰肠吻合口相关并发症的发生率高于研究参与者(P=0.020)。仅内部对照出现死亡。
对于稳定恶性疾病 PD 后的胰肠吻合口,RPTNBD 是一种可行且有效的方法。当 PD 与包括肝切除术或血管重建术在内的技术要求较高的手术联合进行时,RPTNBD 可以预防吻合口的突然失败。