Department of Neurology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan 44033, Korea.
Department of Physical Medicine and Rehabilitation, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan 44033, Korea.
Chin Med J (Engl). 2019 Aug 20;132(16):1919-1924. doi: 10.1097/CM9.0000000000000359.
Differential diagnosis of idiopathic Parkinson disease (IPD) and multiple system atrophy-Parkinson type (MSA-P) is challenging since they share clinical features with parkinsonism and autonomic dysfunction. To distinguish MSA-P from IPD when the symptoms are relatively mild, we investigated the usefulness of the quantitative fractionalized autonomic indexes and evaluated the correlations of autonomic test indexes and functional status.
Thirty-six patients with parkinsonism (22 with IPD and 14 with MSA-P) in Soonchunhyang University Bucheon Hospital from February 2014 to June 2015 were prospectively enrolled in the study. We compared fractionalized autonomic indexes and composite autonomic scoring scale between patients with IPD and MSA-P with Hoehn and Yahr (H&Y) score ≤3. Parasympathetic indexes included expiratory/inspiratory ratio during deep breathing, Valsalva ratio (VR), and regression slope of systolic blood pressure (BP) in early phase II (vagal baroreflex sensitivity) during Valsalva maneuver. Sympathetic adrenergic indexes were pressure recovery time (PRT) and adrenergic baroreflex sensitivity (BRSa) (BP decrement associated with phase 3 divided by the PRT), sympathetic index 1, sympathetic index 3, early phase II mean BP drop, and pulse pressure reduction rate. Additionally, we compared the unified multiple system atrophy rating scale (UMSARS) and H&Y scores and the autonomic indexes in all patients.
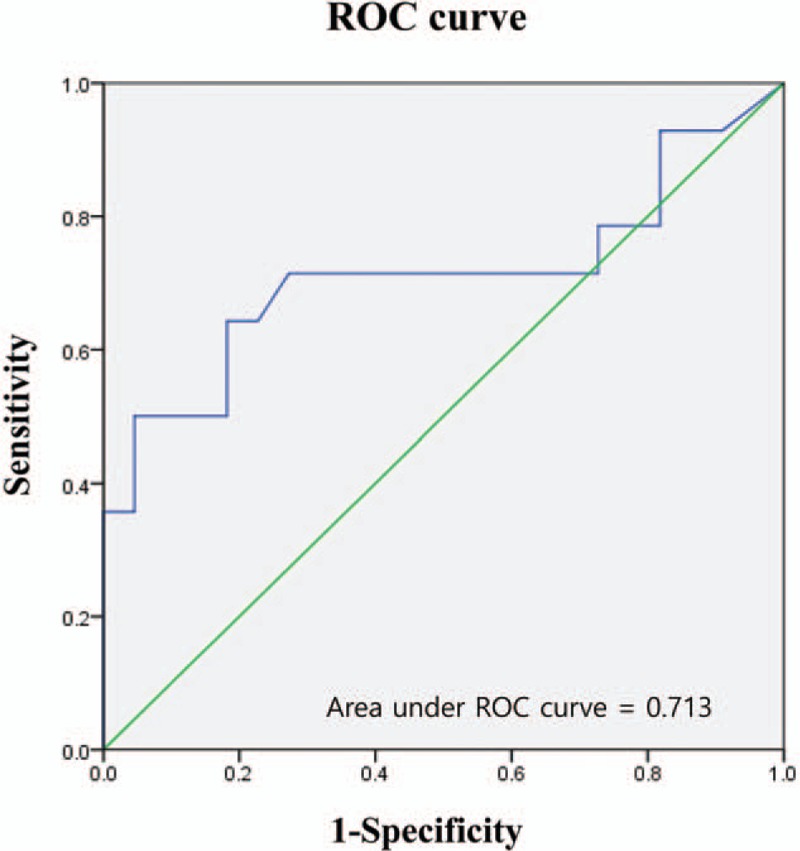
PRT was significantly different between the IPD and MSA-P groups (P = 0.004) despite the similar BP drop during tilt. Cut-off value of PRT was 5.5 s (sensitivity, 71.4%; specificity, 72.7%). VR (r = -0.455, P = 0.009) and BRSa (r = -0.356, P = 0.036) demonstrated a significant correlation with UMSARS and H&Y scores.
Among the cardiovascular autonomic indexes, PRT can be a useful parameter in differentiating the early stage of MSA-P from that of IPD. Moreover, VR, and BRSa may be the optimal indexes in determining functional symptom severity.
特发性帕金森病(IPD)和多系统萎缩-帕金森型(MSA-P)的鉴别诊断具有挑战性,因为它们与帕金森病和自主神经功能障碍具有共同的临床特征。为了在症状相对较轻时区分 MSA-P 和 IPD,我们研究了定量分数化自主神经指数的有用性,并评估了自主神经测试指标与功能状态的相关性。
2014 年 2 月至 2015 年 6 月,我们前瞻性地纳入了在顺天乡大学盆唐医院的 36 名帕金森病患者(22 名 IPD 和 14 名 MSA-P)。我们比较了 IPD 和 MSA-P 患者的分数化自主神经指数和综合自主评分量表与 Hoehn 和 Yahr(H&Y)评分≤3。副交感神经指数包括深吸气/呼气比、瓦尔萨尔瓦比率(VR)和瓦尔萨尔瓦动作期间收缩压(BP)早期阶段 II 的回归斜率(迷走神经压力反射敏感性)。交感神经肾上腺素能指数为压力恢复时间(PRT)和肾上腺素能压力反射敏感性(BRSa)(与第 3 期相关的 BP 下降除以 PRT)、交感神经指数 1、交感神经指数 3、早期阶段 II 平均 BP 下降和脉搏压降低率。此外,我们比较了所有患者的统一多系统萎缩评分量表(UMSARS)和 H&Y 评分以及自主神经指数。
尽管倾斜时的 BP 下降相似,但 IPD 和 MSA-P 组之间的 PRT 差异具有统计学意义(P=0.004)。PRT 的截断值为 5.5s(灵敏度,71.4%;特异性,72.7%)。VR(r=-0.455,P=0.009)和 BRSa(r=-0.356,P=0.036)与 UMSARS 和 H&Y 评分呈显著相关。
在心血管自主神经指数中,PRT 可作为区分 MSA-P 和 IPD 早期阶段的有用参数。此外,VR 和 BRSa 可能是确定功能症状严重程度的最佳指标。