Division of Cardiology, Heart Center, Konyang University Hospital, 158, Gwanjeodong-Ro, Seo-Gu, Daejeon, 35365, South Korea.
BMC Cardiovasc Disord. 2019 Aug 5;19(1):187. doi: 10.1186/s12872-019-1173-5.
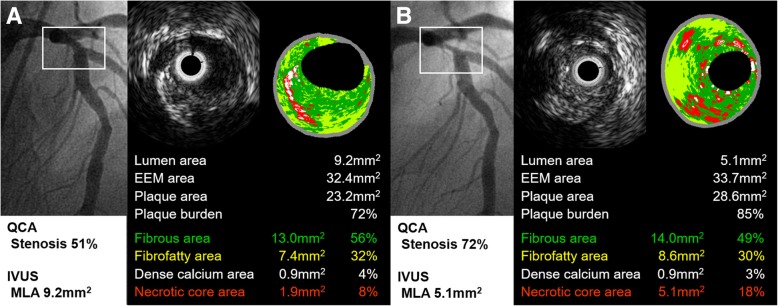
It is uncertain whether the coronary lesion with intermediate stenosis is more likely to cause cardiovascular events than a normal or minimal lesion. We conducted a single-center, prospective cohort study to identify long-term clinical outcomes of patients with untreated non-culprit intermediate lesion and evaluate its predictor of cardiovascular events by using virtual histology-intravascular ultrasound (VH-IVUS).
Subjects with non-culprit intermediate lesion underwent VH-IVUS were prospectively registered after percutaneous coronary intervention at the culprit lesion. Intermediate lesion was defined as 30 to 70% stenosis in coronary angiography and primary outcome was an occurrence of major adverse cardiovascular events (MACE) defined as all-cause death, intermediate lesion revascularization (InLR), minimal lesion revascularization (MnLR, unplanned revascularization elsewhere in the target vessel or in other coronary arteries which looked normal or minimal stenosis), cerebrovascular events, or non-fatal myocardial infarction (MI). The mean follow-up period was 4.2 years.
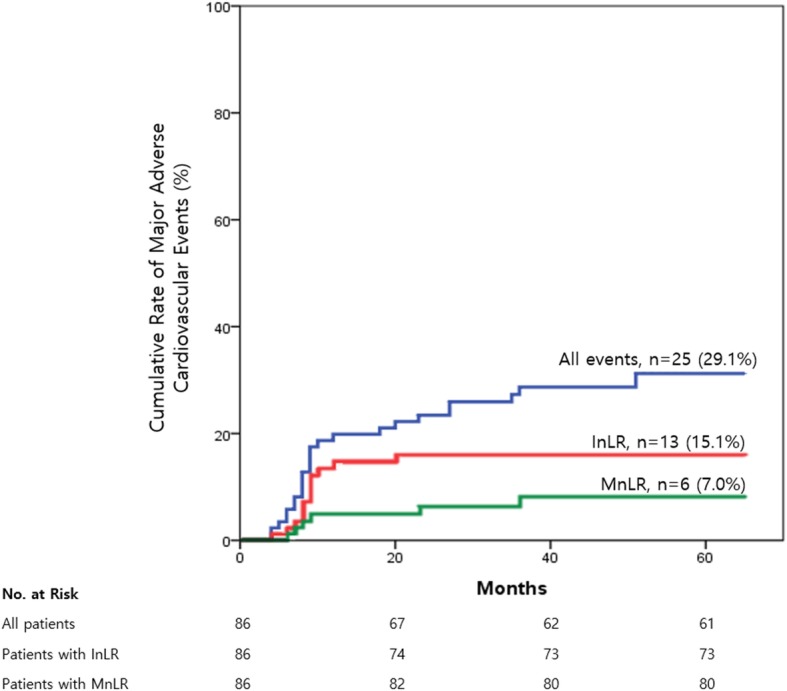
Total 25 MACE, approximately 7% incidence annually, were identified during a follow-up period in 86 patients with 89 intermediate lesions. InLR (n = 13) was a most common event followed by MnLR (n = 6), non-fatal MI (n = 4), all-cause death (n = 3), and cerebrovascular events (n = 1). Diameter stenosis (OR 1.07, 95% CI 1.01-1.12, p = 0.015), plaque burden (PB, OR 1.07, 95% CI 1.00-1.15, p = 0.040), fibrofatty area (FFA, OR 1.61, 95% CI 1.10-2.38, p = 0.016), PB ≥ 70% (OR 3.93, 95% CI 1.28-12.07, p = 0.018), and area stenosis ≥ 50% (OR 2.94, 95% CI 1.01-8.56, p = 0.042) showed significant relationships with an occurrence of MACE. In multivariable Cox-proportional hazard analysis, FFA in intermediate lesion was an only independent predictor of MACE (HR 1.36, 95% CI 1.05-1.77, p = 0.019).
Untreated intermediate lesions had a significantly higher chance for requiring revascularization compared with a normal or minimal lesion. And also, a large FFA in intermediate lesion was a significant predictor of cardiovascular events and which finding was mainly driven by coronary-related events, in particularly intermediate lesion progression.
介于临界值的狭窄冠状动脉病变与正常或轻微病变相比,是否更易引发心血管事件还不确定。我们进行了一项单中心前瞻性队列研究,旨在通过虚拟组织学血管内超声(VH-IVUS)识别未经治疗的非罪犯性中间病变患者的长期临床结局,并评估其心血管事件的预测因素。
经皮冠状动脉介入治疗罪犯病变后,对中间病变行 VH-IVUS 检查的非罪犯性中间病变患者被前瞻性登记。中间病变定义为冠状动脉造影狭窄 30%至 70%,主要终点为主要不良心血管事件(MACE)的发生,MACE 定义为全因死亡、中间病变血运重建(InLR)、微小病变血运重建(MnLR,目标血管或其他看起来正常或狭窄程度轻微的冠状动脉内的计划性血运重建)、脑血管事件或非致命性心肌梗死(MI)。中位随访时间为 4.2 年。
在 86 例患者的 89 个中间病变中,共发现 25 例 MACE,每年约 7%的发生率。InLR(n=13)是最常见的事件,其次是 MnLR(n=6)、非致命性 MI(n=4)、全因死亡(n=3)和脑血管事件(n=1)。直径狭窄(OR 1.07,95%CI 1.01-1.12,p=0.015)、斑块负荷(PB,OR 1.07,95%CI 1.00-1.15,p=0.040)、纤维脂肪面积(FFA,OR 1.61,95%CI 1.10-2.38,p=0.016)、PB≥70%(OR 3.93,95%CI 1.28-12.07,p=0.018)和面积狭窄≥50%(OR 2.94,95%CI 1.01-8.56,p=0.042)与 MACE 的发生显著相关。多变量 Cox 比例风险分析显示,中间病变中的 FFA 是 MACE 的唯一独立预测因子(HR 1.36,95%CI 1.05-1.77,p=0.019)。
未经治疗的中间病变与正常或轻微病变相比,需要血运重建的可能性明显更高。此外,中间病变中较大的 FFA 是心血管事件的显著预测因子,这一发现主要是由与冠状动脉相关的事件驱动的,特别是中间病变的进展。