Department of Pneumology and Critical Care Medicine, Cologne-Merheim Hospital, Kliniken der Stadt Köln GmbH, Witten/Herdecke University Hospital, Ostmerheimer Strasse 200, D-51109, Cologne, Germany.
Dept of Intensive Care Medicine, Amsterdam UMC, location VUmc, Amsterdam, The Netherlands.
BMC Anesthesiol. 2019 Aug 9;19(1):147. doi: 10.1186/s12871-019-0824-5.
The current study investigates the effect of bronchoscopy-guided percutaneous dilatational tracheostomy (PDT) on the evolution of respiratory acidosis depending on endotracheal tube (ET) sizes. In addition, the impact of increasing tidal volumes during the intervention was investigated.
Two groups of ICU-patients undergoing bronchoscopy-guided PDT with varying tidal volumes and tube sizes were consecutively investigated: 6 ml/kg (N = 29, mean age 57.4 ± 14.5 years) and 12 ml/kg predicted body weight (N = 34, mean age 59.5 ± 12.8 years).
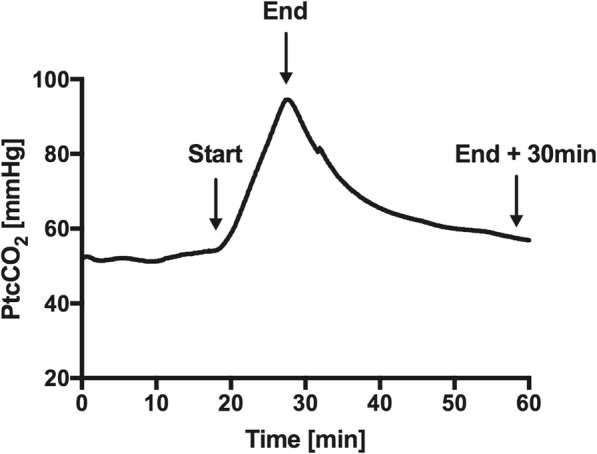
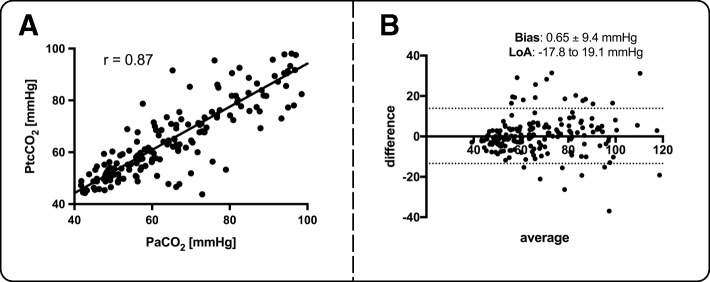
The mean intervention time during all procedures was 10 ± 3 min. The combination of low tidal volumes and ETs of 7.5 mm internal diameter resulted in the most profound increase in PaCO (32.2 ± 11.6 mmHg) and decrease in pH-value (- 0.18 ± 0.05). In contrast, the combination of high tidal volumes and ETs of 8.5 mm internal diameter resulted in the least profound increase in PaCO (8.8 ± 9.0 mmHg) and decrease of pH (- 0.05 ± 0.04). The intervention-related increase in PaCO was significantly lower when using higher tidal volumes for larger ET: internal diameter 7.5, 8.0 and 8.5: P > 0.05, =0.006 and = 0.002, respectively. Transcutaneous PCO monitoring revealed steadily worsening hypercapnia during the intervention with a high correlation of 0.87 and a low bias of 0.7 ± 9.4 mmHg according to the Bland-Altman analysis when compared to PaCO measurements.
Profound respiratory acidosis following bronchoscopy-guided PDT evolves in a rapid and dynamic process. Increasing the tidal volume from 6 to 12 ml/kg PBW was capable of attenuating the evolution of respiratory acidosis, but this effect was only evident when using larger ETs.
DRKS00011004 . Registered 20th September 2016.
本研究旨在探讨支气管镜引导下经皮扩张气管切开术(PDT)对不同气管内导管(ET)大小下呼吸性酸中毒演变的影响。此外,还研究了干预过程中潮气量增加的影响。
连续研究了两组在支气管镜引导下进行 PDT 的 ICU 患者,潮气量和导管大小不同:6ml/kg(N=29,平均年龄 57.4±14.5 岁)和 12ml/kg 预测体重(N=34,平均年龄 59.5±12.8 岁)。
所有操作的平均干预时间为 10±3min。低潮气量和 7.5mm 内径的 ET 联合使用导致 PaCO2 升高最明显(32.2±11.6mmHg),pH 值下降最明显(-0.18±0.05)。相比之下,高潮气量和 8.5mm 内径的 ET 联合使用导致 PaCO2 升高最不明显(8.8±9.0mmHg),pH 值下降最不明显(-0.05±0.04)。当使用更大的 ET 时,潮气量越高,干预相关的 PaCO2 升高越低:内径 7.5、8.0 和 8.5:P>0.05,=0.006 和=0.002。经皮 PCO 监测显示,在干预过程中,二氧化碳分压逐渐升高,与 PaCO2 测量值相比,相关性为 0.87,偏差为 0.7±9.4mmHg,具有低偏倚。
支气管镜引导下 PDT 后呼吸性酸中毒迅速而动态地发展。将潮气量从 6 增加到 12ml/kg PBW 能够减轻呼吸性酸中毒的演变,但只有在使用更大的 ET 时才会出现这种效果。
DRKS00011004。2016 年 9 月 20 日注册。