Jayaprakash Namita, Chae Junemee, Sabov Moldovan, Samavedam Sandhya, Gajic Ognjen, Pickering Brian W
Department of Emergency Medicine, Henry Ford Hospital, Detroit, MI.
Division of Pulmonary and Critical Care, Henry Ford Hospital, Detroit, MI.
Mayo Clin Proc Innov Qual Outcomes. 2019 Jul 19;3(3):327-334. doi: 10.1016/j.mayocpiqo.2019.06.001. eCollection 2019 Sep.
To reliably improve diagnostic fidelity and identify delays using a standardized approach applied to the electronic medical records of patients with emerging critical illness.
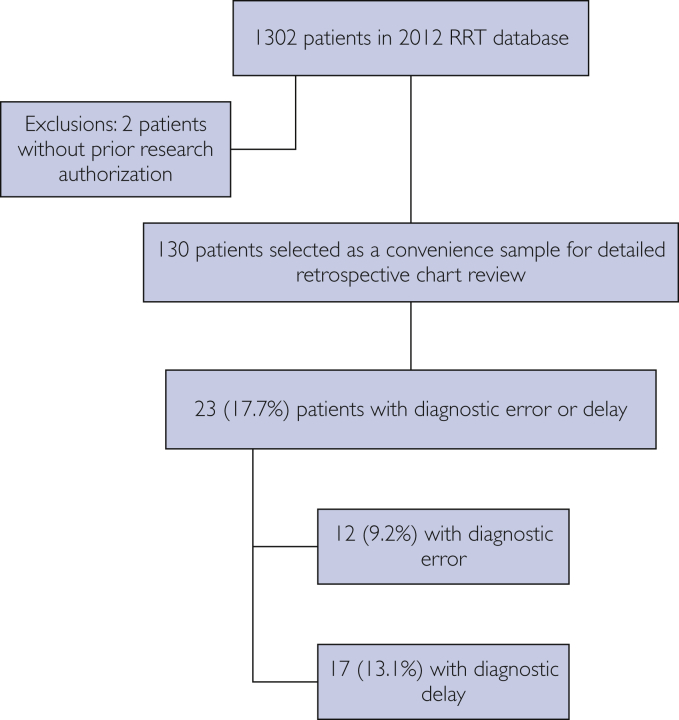
This retrospective observational study at Mayo Clinic, Rochester, Minnesota, conducted June 1, 2016, to June 30, 2017, used a standard operating procedure applied to electronic medical records to identify variations in diagnostic fidelity and/or delay in adult patients with a rapid response team evaluation, at risk for critical illness. Multivariate logistic regression analysis identified predictors and compared outcomes for those with and without varying diagnostic fidelity and/or delay.
The sample included 130 patients. Median age was 65 years (interquartile range, 56-76 years), and 47.0% (52 of 130) were women. Clinically significant diagnostic error or delay was agreed in 23 (17.7%) patients (κ=0.57; 95% CI, 0.40-0.74). Median age was 65.4 years (interquartile range, 60.3-74.8) and 9 of the 23 (30.1%) were female. Of those with diagnostic error or delay, 60.9% (14 of 23) died in the hospital compared with 19.6% (21 of 107) without; <.001. Diagnostic error or delay was associated with higher Charlson comorbidity index score, cardiac arrest triage score, and do not intubate/do not resuscitate status. Adjusting for age, do not intubate/do not resuscitate status, and Charlson comorbidity index score, diagnostic error or delay was associated with increased mortality; odds ratio, 5.7; 95% CI, 2.0-17.8.
Diagnostic errors or delays can be reliably identified and are associated with higher comorbidity burden and increased mortality.
采用标准化方法应用于危重症初发患者的电子病历,以可靠地提高诊断准确性并识别诊断延迟。
这项于2016年6月1日至2017年6月30日在明尼苏达州罗切斯特市梅奥诊所进行的回顾性观察研究,使用了应用于电子病历的标准操作程序,以识别在快速反应团队评估中存在危重症风险的成年患者的诊断准确性差异和/或诊断延迟。多因素逻辑回归分析确定了预测因素,并比较了诊断准确性不同和/或存在诊断延迟与不存在这些情况的患者的结局。
样本包括130名患者。中位年龄为65岁(四分位间距,56 - 76岁),47.0%(130名中的52名)为女性。23名(17.7%)患者存在具有临床意义的诊断错误或延迟(κ = 0.57;95%置信区间,0.40 - 0.74)。中位年龄为65.4岁(四分位间距,60.3 - 74.8),23名中的9名(30.1%)为女性。在存在诊断错误或延迟的患者中,60.9%(23名中的14名)在医院死亡,而无诊断错误或延迟的患者中这一比例为19.6%(107名中的21名);P <.001。诊断错误或延迟与较高的查尔森合并症指数评分、心脏骤停分诊评分以及不插管/不复苏状态相关。在对年龄、不插管/不复苏状态和查尔森合并症指数评分进行校正后,诊断错误或延迟与死亡率增加相关;比值比为5.7;95%置信区间,2.0 - 17.8。
诊断错误或延迟能够被可靠地识别,并且与更高的合并症负担和死亡率增加相关。