Cai He, Zheng Yang, Liu Zhaoxi, Zhang Xinying, Li Rongyu, Shao Wangshu, Wang Lin, Zou Lin, Cao Pengyu
The Cardiovascular Center, First Hospital of Jilin University, 71 Xinmin Road, Changchun, 130021, Jilin, China.
BMC Cardiovasc Disord. 2019 Sep 6;19(1):210. doi: 10.1186/s12872-019-1189-x.
The purpose of this study was to analyze cardiopulmonary fitness in Phase I cardiac rehabilitation on the prognosis of patients with ST-Elevation Myocardial Infarction (STEMI) after percutaneous coronary intervention (PCI).
The study enrolled a total of 499 STEMI patients treated with PCI between January 2015 and December 2015. Patients were assigned to individualized exercise prescriptions (IEP) group and non-individualized exercise prescriptions (NIEP) group according to whether they accept or refuse individualized exercise prescriptions. We compared the incidence of major cardiovascular events between the two groups. IEP group were further divided into two subgroups based on prognosis status, namely good prognosis (GP) group and poor prognosis (PP) group. Key cardio-pulmonary exercise testing (CPX) variables that may affect the prognosis of patients were identified through comparison of the cardio-respiratory fitness (CRF).
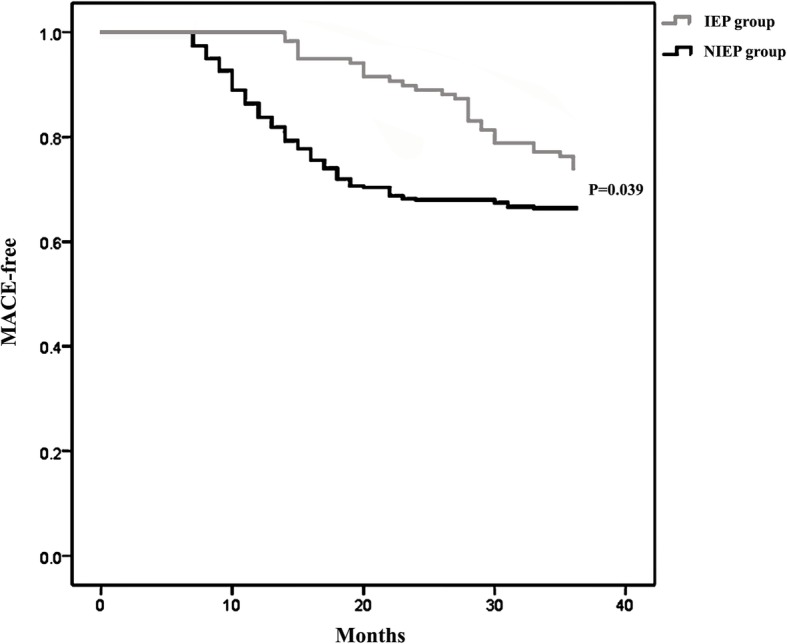
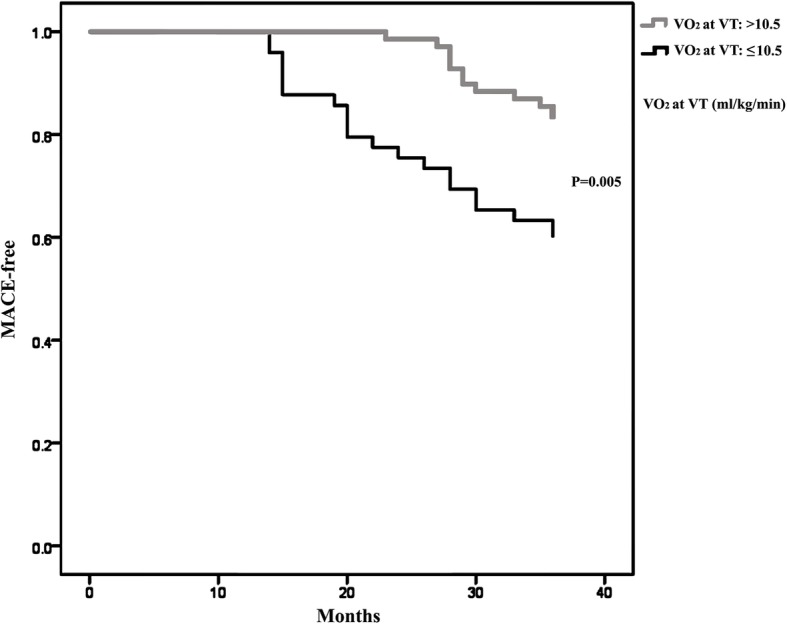
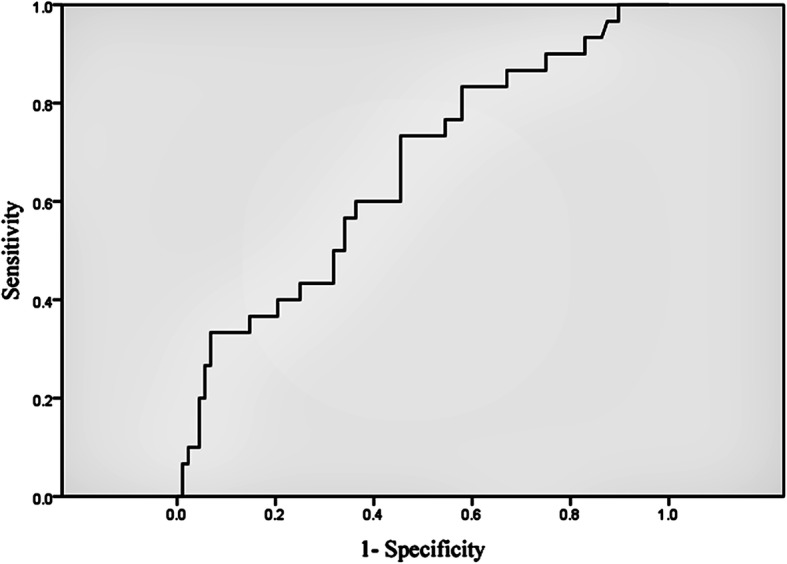
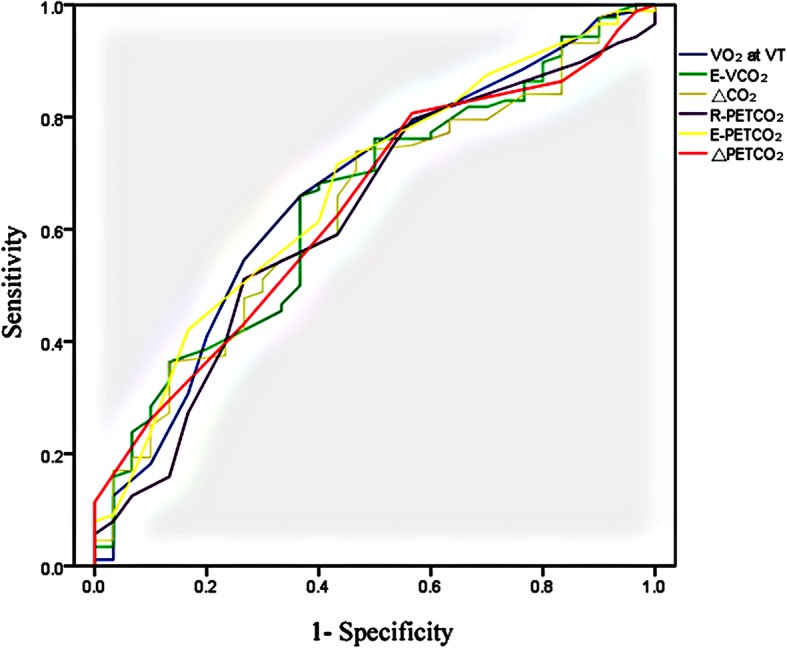
There is no significant difference in the incidence of cardio-genetic death, re-hospitalization, heart failure, stroke, or atrial fibrillation between the IEP and the NIEP group. But the incidence of total major adverse cardiac events (MACE) was significantly lower in the IEP group than in the NIEP group (P = 0.039). The oxygen consumption (VO) at ventilation threshold (VT), minute CO ventilation (E-VCO), margin of minute ventilation carbon dioxide production (△CO) rest partial pressure of end-tidal carbon dioxide(R-PCO), exercise partial pressure of end-tidal carbon dioxide(E-PCO) and margin of partial pressure of end-tidal carbon dioxide(△PCO) were significantly higher in the GP subgroup than in the PP subgroup; and the slope for minute ventilation/carbon dioxide production (V/VCO) was significantly lower in GP subgroup than in PP subgroup (P = 0.010). The VO at VT, V/VCO slope, E-VCO, △CO, R-PCO, E-PCO and margin of partial pressure of end-tidal carbon dioxide CO (△PCO) were predictive of adverse events. The VO at VT was an independent risk factor for cardiovascular disease prognosis.
Individualized exercise prescription of Phase I cardiac rehabilitation reduced the incidence of cardiovascular events in patients with STEMI after PCI. VO at VT is an independent risk factor for cardiovascular disease prognosis, and could be used as an important evaluating indicator for Phase I cardiac rehabilitation.
本研究旨在分析I期心脏康复中的心肺适能对接受经皮冠状动脉介入治疗(PCI)的ST段抬高型心肌梗死(STEMI)患者预后的影响。
本研究纳入了2015年1月至2015年12月期间共499例接受PCI治疗的STEMI患者。根据患者是否接受个体化运动处方,将其分为个体化运动处方(IEP)组和非个体化运动处方(NIEP)组。我们比较了两组主要心血管事件的发生率。IEP组根据预后状况进一步分为两个亚组,即预后良好(GP)组和预后不良(PP)组。通过比较心肺适能(CRF),确定了可能影响患者预后的关键心肺运动试验(CPX)变量。
IEP组和NIEP组在心源性死亡、再次住院、心力衰竭、中风或房颤的发生率上无显著差异。但IEP组总的主要不良心脏事件(MACE)发生率显著低于NIEP组(P = 0.039)。通气阈值(VT)时的耗氧量(VO)、分钟二氧化碳通气量(E-VCO)、分钟通气量与二氧化碳产生量的差值(△CO)、静息呼气末二氧化碳分压(R-PCO)、运动呼气末二氧化碳分压(E-PCO)和呼气末二氧化碳分压差值(△PCO)在GP亚组中显著高于PP亚组;而GP亚组的分钟通气量/二氧化碳产生量斜率(V/VCO)显著低于PP亚组(P = 0.010)。VT时的VO、V/VCO斜率、E-VCO、△CO、R-PCO、E-PCO和呼气末二氧化碳分压差值(△PCO)可预测不良事件。VT时的VO是心血管疾病预后的独立危险因素。
I期心脏康复的个体化运动处方降低了PCI术后STEMI患者心血管事件的发生率。VT时的VO是心血管疾病预后的独立危险因素,可作为I期心脏康复的重要评估指标。