Hessey Erin, Perreault Sylvie, Dorais Marc, Roy Louise, Zappitelli Michael
Division of Nephrology, Department of Pediatrics, Montreal Children's Hospital, McGill University Health Centre, QC, Canada.
Faculty of Pharmacy, Université de Montréal, QC, Canada.
Can J Kidney Health Dis. 2019 Oct 14;6:2054358119880188. doi: 10.1177/2054358119880188. eCollection 2019.
The progression from acute kidney injury (AKI) to chronic kidney disease (CKD) is not well understood in children.
We aimed to develop a pediatric CKD definition using administrative data and use it to evaluate the association between AKI in critically ill children and CKD 5 years after hospital discharge.
Retrospective cohort study using chart collection and administrative data.
Two-center study in Montreal, Canada.
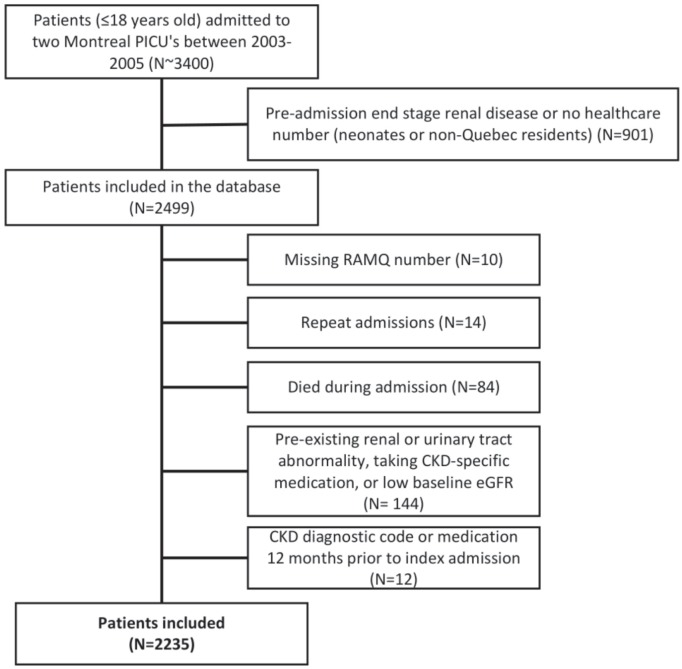
Children (≤18 years old) admitted to two pediatric intensive care units (ICUs) between 2003 and 2005. We a priori excluded patients with end-stage renal disease or no health care number. Only the first admission during the study period was included. We excluded patients who could not be linked to administrative data, did not survive hospitalization, or had preexisting renal disease.
Acute kidney injury was defined using Kidney Disease: Improving Global Outcomes (KDIGO) criteria. Patients were defined as having CKD 5 years post-discharge if they had ≥1 CKD diagnostic code or ≥1 CKD-specific medication prescription.
Chart data used to define the exposure (AKI) were merged with provincial administrative data used to define the outcome (CKD). Cox regression was used to evaluate the AKI-CKD association.
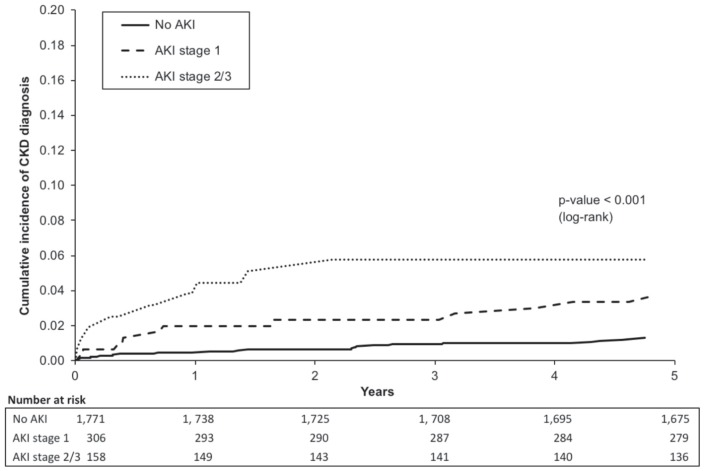
A total of 2235 (56% male) patients were included, and the median admission age was 3.7 years. A total of 464 (21%) patients developed AKI during pediatric ICU admission. At 5 years post-discharge, 43 (2%) patients had a CKD diagnosis. Patients with both stage 1 and stage 2-3 AKI had increased risk of a CKD diagnosis, with the adjusted hazard ratios (95% confidence intervals) of 2.2 (1.1-4.5) and 2.5 (1.1-5.7), respectively ( < .001).
Results may not be generalizable to non-ICU patients. We were not able to control for post-discharge variables; future research should try to explore these additional potential risk factors further.
Acute kidney injury is associated with 5-year post-discharge CKD diagnosis defined by administrative health care data.
儿童从急性肾损伤(AKI)进展为慢性肾脏病(CKD)的情况尚未完全明确。
我们旨在利用行政数据制定儿童CKD的定义,并使用该定义评估危重症儿童AKI与出院后5年CKD之间的关联。
采用图表收集和行政数据的回顾性队列研究。
加拿大蒙特利尔的双中心研究。
2003年至2005年间入住两个儿科重症监护病房(ICU)的儿童(≤18岁)。我们事先排除了终末期肾病患者或无医疗保健编号的患者。仅纳入研究期间的首次入院患者。我们排除了无法与行政数据关联、住院期间未存活或有既往肾病的患者。
急性肾损伤采用《肾脏病:改善全球预后》(KDIGO)标准进行定义。如果患者有≥1个CKD诊断代码或≥1个CKD特异性药物处方,则定义为出院后5年患有CKD。
用于定义暴露因素(AKI)的图表数据与用于定义结局(CKD)的省级行政数据合并。采用Cox回归评估AKI与CKD的关联。
共纳入2235例患者(56%为男性),中位入院年龄为3.7岁。共有464例(21%)患者在儿科ICU住院期间发生AKI。出院后5年,43例(2%)患者被诊断为CKD。1期和2 - 3期AKI患者的CKD诊断风险均增加,校正风险比(95%置信区间)分别为2.2(1.1 - 4.5)和2.5(1.1 - 5.7)(P <.001)。
结果可能不适用于非ICU患者。我们无法控制出院后的变量;未来研究应进一步探索这些额外的潜在危险因素。
急性肾损伤与行政医疗保健数据定义的出院后5年CKD诊断相关。