Center for Innovation to Implementation, VA Palo Alto Healthcare System, 795 Willow Road, Menlo Park, CA, 94025, USA.
Program Evaluation and Resource Center, VA Office of Mental Health and Suicide Prevention, Menlo Park, CA, USA.
J Gen Intern Med. 2020 Apr;35(4):1044-1051. doi: 10.1007/s11606-019-05410-y. Epub 2019 Dec 12.
Clinical practice guidelines suggest that magnetic resonance imaging of the lumbar spine (LS-MRI) is unneeded during the first 6 weeks of acute, uncomplicated low-back pain. Unneeded LS-MRIs do not improve patient outcomes, lead to unnecessary surgeries and procedures, and cost the US healthcare system about $300 million dollars per year. However, why primary care providers (PCPs) order unneeded LS-MRI for acute, uncomplicated low-back pain is poorly understood.
To characterize and explain the factors contributing to PCPs ordering unneeded LS-MRI for acute, uncomplicated low-back pain.
Qualitative study using semi-structured interviews.
Veterans Affairs PCPs identified from administrative data as having high or low rates of guideline-concordant LS-MRI ordering in 2016.
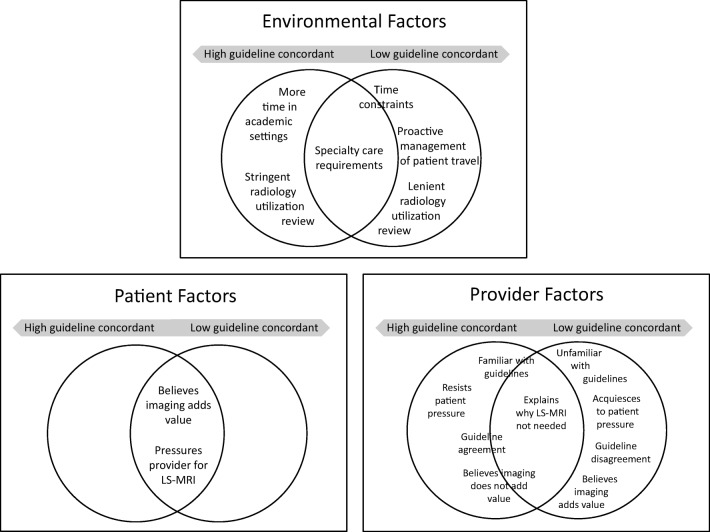
Providers were interviewed about their use of LS-MRI for acute, uncomplicated low-back pain and factors contributing to their decision-making. Directed content analysis of transcripts was conducted to identify and compare environmental-, patient-, and provider-level factors contributing to unneeded LS-MRI.
Fifty-five PCPs participated (8.6% response rate). Both low (n = 33) and high (n = 22) guideline-concordant providers reported that LS-MRIs were required for specialty care referrals, but they differed in how other environmental factors (stringency of radiology utilization review, management of patient travel burden, and time constraints) contributed to LS-MRI ordering patterns. Low- and high-guideline-concordant providers reported similar patient factors (beliefs in value of imaging and pressure on providers). However, provider groups differed in how provider-level factors (guideline familiarity and agreement, the extent to which they acquiesced to patients, and belief in the value of LS-MRI) contributed to LS-MRI ordering patterns.
Results describe how diverse environmental, patient, and provider factors contribute to unneeded LS-MRI for acute, uncomplicated low-back pain. Prior research using a single intervention to reduce unneeded LS-MRI has been ineffective. Results suggest that multifaceted de-implementation strategies may be required to reduce unneeded LS-MRI.
临床实践指南建议,在急性、单纯性下背痛的最初 6 周内,腰椎磁共振成像(LS-MRI)无必要。不必要的 LS-MRI 不会改善患者的结局,反而会导致不必要的手术和程序,并使美国医疗保健系统每年损失约 3 亿美元。然而,初级保健提供者(PCP)为何会为急性、单纯性下背痛开出不必要的 LS-MRI 还了解甚少。
描述和解释导致 PCP 为急性、单纯性下背痛开出不必要的 LS-MRI 的因素。
使用半结构式访谈的定性研究。
从 2016 年的管理数据中确定的 VA PCP,其 LS-MRI 符合指南的开单率较高或较低。
对提供者进行关于他们对急性、单纯性下背痛使用 LS-MRI 以及促成其决策的因素的访谈。对转录本进行定向内容分析,以识别和比较促成不必要 LS-MRI 的环境、患者和提供者层面的因素。
55 名 PCP 参与(8.6%的回应率)。低(n=33)和高(n=22)符合指南的提供者都报告说,LS-MRI 是专科治疗转诊所必需的,但他们在其他环境因素(放射学利用审查的严格程度、患者旅行负担的管理以及时间限制)如何促成 LS-MRI 开单模式方面存在差异。低和高符合指南的提供者报告了类似的患者因素(对影像学价值的信念和对提供者的压力)。然而,提供者群体在提供者层面的因素(对指南的熟悉程度和认同程度、他们对患者的顺从程度以及对 LS-MRI 的价值的信念)如何促成 LS-MRI 开单模式方面存在差异。
结果描述了不同的环境、患者和提供者因素如何促成急性、单纯性下背痛的不必要 LS-MRI。以前使用单一干预措施来减少不必要的 LS-MRI 的研究没有效果。结果表明,可能需要多方面的去实施策略来减少不必要的 LS-MRI。