Department of Surgery, Duke University Medical Center, Box 3513, Durham, NC, 27710, USA.
Women's Cancer Program, Duke Cancer Institute, Durham, NC, 27710, USA.
Breast Cancer Res Treat. 2020 Feb;180(1):207-217. doi: 10.1007/s10549-020-05529-1. Epub 2020 Jan 20.
Inflammatory breast cancer (IBC) is an aggressive variant for which axillary lymph node (LN) dissection following neoadjuvant chemotherapy (NACT) remains standard of care. But with increasingly effective systemic therapy, it is unclear whether more limited axillary surgery may be appropriate in some IBC patients. We sought to examine whether extent of axillary LN surgery was associated with overall survival (OS) for IBC.
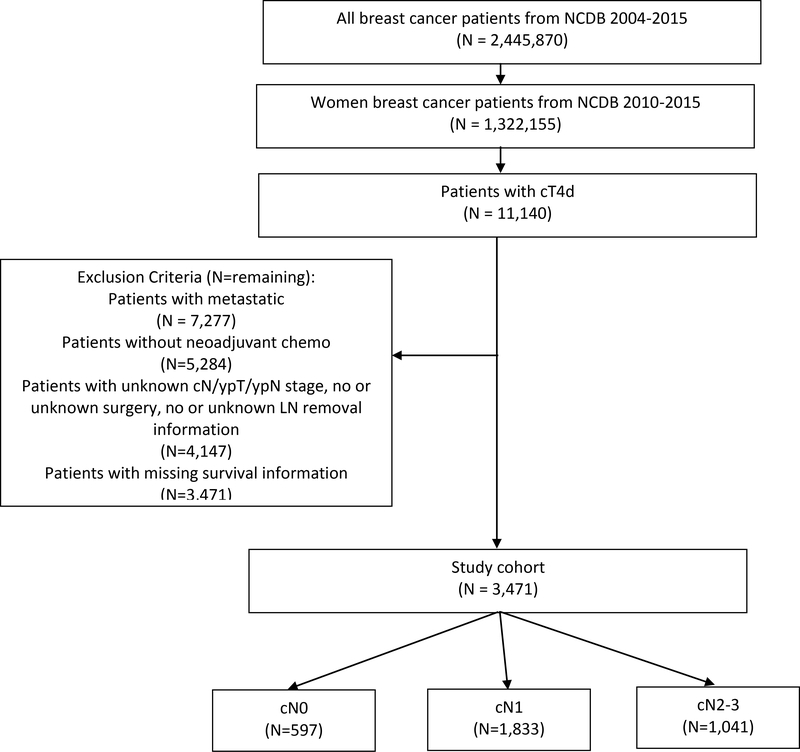
Female breast cancer patients with non-metastatic IBC (cT4d) diagnosed 2010-2014 were identified in the National Cancer Data Base. Cox proportional hazards modeling was used to estimate the association between extent of axillary surgery (≤ 9 vs ≥ 10 LNs removed) and OS after adjusting for covariates, including post-NACT nodal status (ypN0 vs ypN1-3) and radiotherapy receipt (yes/no).
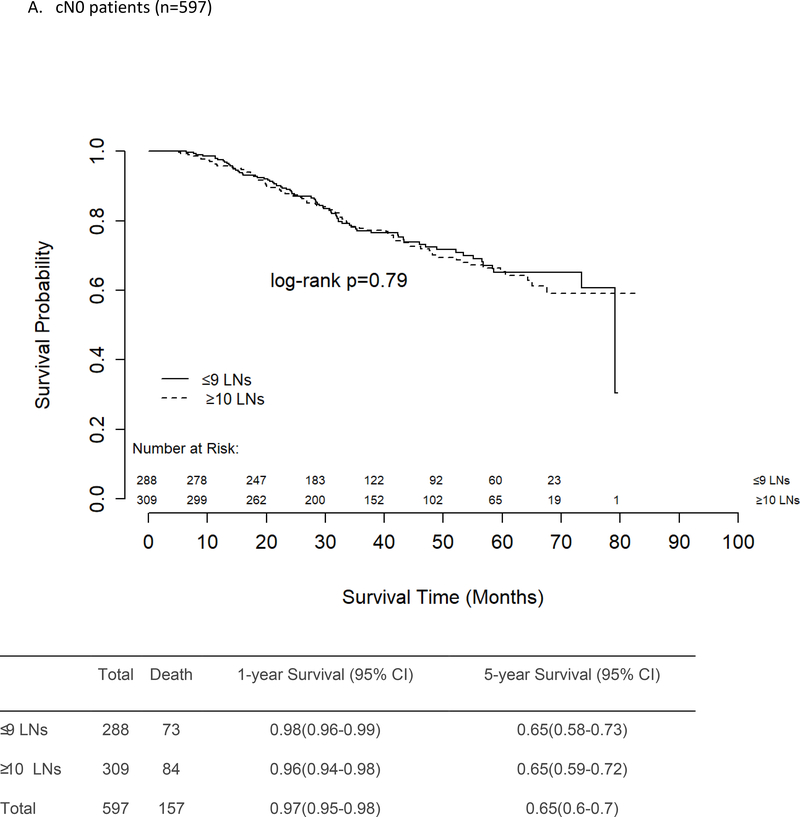
3471 patients were included: 597 (17.2%) had cN0 disease, 1833 (52.8%) had cN1 disease, and 1041 (30%) had cN2-3 disease. 49.9% of cN0 patients were confirmed to be ypN0 on post-NACT surgical pathology. Being ypN0 (vs ypN1-3) was associated with improved adjusted OS for all patients. Radiotherapy was associated with improved adjusted OS for cN1 and cN2-3 patients but not for cN0 patients. Regardless of ypN status, there was a trend towards improved adjusted OS with having ≥ 10 (vs ≤ 9) LNs removed for cN2-3 patients (HR 0.78, 95% CI 0.60-1.01, p = 0.06) but not for cN0 patients (p = 0.83).
A majority of IBC patients in our study presented with node-positive disease, and for those presenting with cN2-3 disease, more extensive axillary surgery is potentially associated with improved survival. For cN0 patients, however, more extensive axillary surgery was not associated with a survival benefit, suggesting an opportunity for more personalized care.
炎性乳腺癌(IBC)是一种侵袭性较强的乳腺癌,新辅助化疗(NACT)后行腋窝淋巴结(LN)清扫仍然是标准治疗方案。但随着系统治疗越来越有效,在某些 IBC 患者中,更有限的腋窝手术是否合适仍不清楚。我们试图研究腋窝 LN 手术范围是否与 IBC 的总生存(OS)相关。
在国家癌症数据库中,确定了 2010-2014 年诊断为非转移性 IBC(cT4d)的女性乳腺癌患者。使用 Cox 比例风险模型估计腋窝手术范围(≤9 个 vs ≥10 个 LN 切除)与 OS 之间的关系,调整了包括新辅助化疗后淋巴结状态(ypN0 与 ypN1-3)和放疗(是/否)在内的协变量。
共纳入 3471 例患者:597 例(17.2%)为 cN0 疾病,1833 例(52.8%)为 cN1 疾病,1041 例(30%)为 cN2-3 疾病。49.9%的 cN0 患者在新辅助化疗后的手术病理中确认为 ypN0。对于所有患者,ypN0(与 ypN1-3 相比)与调整后的 OS 改善相关。放疗与 cN1 和 cN2-3 患者的调整后 OS 改善相关,但与 cN0 患者无关。无论 ypN 状态如何,对于 cN2-3 患者,切除≥10(与≤9)个 LN 与调整后的 OS 改善趋势相关(HR 0.78,95%CI 0.60-1.01,p=0.06),但与 cN0 患者无关(p=0.83)。
在我们的研究中,大多数 IBC 患者表现为淋巴结阳性疾病,对于那些表现为 cN2-3 疾病的患者,更广泛的腋窝手术可能与生存改善相关。然而,对于 cN0 患者,更广泛的腋窝手术与生存获益无关,这表明有机会进行更个性化的治疗。