Departments of Medicine & Biochemistry, Division of Gastroenterology and Hepatology, University of New Mexico School of Medicine and Raymond G. Murphy Veterans Administration Medical Center, 1501 San Pedro Blvd. SE, Albuquerque, NM 87108, USA.
Int J Mol Sci. 2020 Jan 19;21(2):662. doi: 10.3390/ijms21020662.
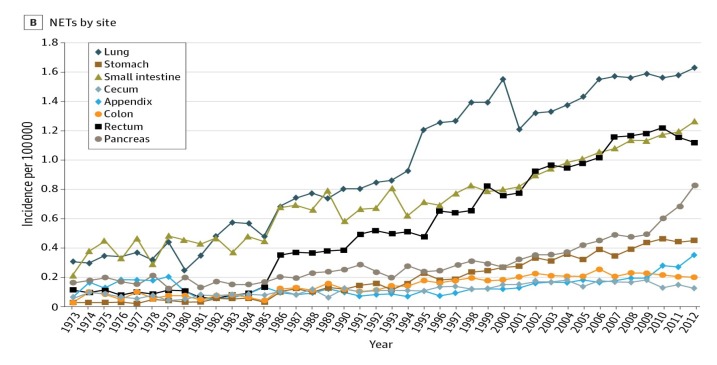
Neuroendocrine tumors (NETs) throughout the body are the focus of much current interest. Most occur in the gastrointestinal tract and have shown a major increase in incidence over the past 30 years, roughly paralleling the world-wide increase in the use of proton pump inhibitor (PPI) drugs. The greatest rise has occurred in gastric carcinoids (g-NETs) arising from enterochromaffin-like (ECL) cells. These tumors are long known to occur in auto-immune chronic atrophic gastritis (CAG) and Zollinger-Ellison syndrome (ZES), with or without multiple endocrine neoplasia type-1 (MEN-1), but the incidences of these conditions do not appear to have increased over the same time period. Common to these disease states is persistent hypergastrinemia, generally accepted as causing g-NETs in CAG and ZES, and postulated as having similar tumorigenic effects in PPI users. In efforts to study the increase in their occurrence, g-NETs have been classified in a number of discussed ways into different grades that differ in their incidence and apparent pathogenesis. Based on a large amount of experimental data, tumorigenesis is mediated by gastrin's effects on the CCK2R-receptor on ECL-cells that in turn leads to hyperplasia, dysplasia, and finally neoplasia. However, in all three conditions, the extent of response of ECL-cells to gastrin is modified by a number of genetic influences and other underlying risk factors, and by the duration of exposure to the hormonal influence. Data relating to trophic effects of hypergastrinemia due to PPI use in humans are reviewed and, in an attached Appendix A, all 11 reports of g-NETs that occurred in long-term PPI users in the absence of CAG or ZES are summarized. Mention of additional suspected cases reported elsewhere are also listed. Furthermore, the risk in humans may be affected by the presence of underlying conditions or genetic factors, including their PPI-metabolizer phenotype, with slow metabolizers likely at increased risk. Other problems in estimating the true incidence of g-NETs are discussed, relating to non-reporting of small tumors and failure of the Surveillance, Epidemiology, and End Results Program (SEER) and other databases, to capture small tumors or those not accorded a T1 rating. Overall, it appears likely that the true incidence of g-NETs may be seriously underestimated: the possibility that hypergastrinemia also affects tumorigenesis in additional gastrointestinal sites or in tumors in other organ systems is briefly examined. Overall, the risk of developing a g-NET appears greatest in patients who are more than 10 years on drug and on higher doses: those affected by chronic gastritis and/or consequent gastric atrophy may also be at increased risk. While the overall risk of g-NETs induced by PPI therapy is undoubtedly low, it is real: this necessitates caution in using PPI therapy for long periods of time, particularly when initiated in young subjects.
全身的神经内分泌肿瘤 (NETs) 是目前研究的重点。大多数 NET 发生在胃肠道,在过去 30 年中,其发病率显著增加,大致与质子泵抑制剂 (PPI) 药物在世界范围内的使用增加相平行。胃类癌 (g-NETs) 的发病率上升最大,起源于肠嗜铬样 (ECL) 细胞。这些肿瘤长期以来一直存在于自身免疫性慢性萎缩性胃炎 (CAG) 和卓-艾综合征 (ZES) 中,无论是否存在多发性内分泌肿瘤 1 型 (MEN-1),但这些疾病的发病率在同一时期似乎并没有增加。这些疾病状态的共同点是持续性高胃泌素血症,一般认为 CAG 和 ZES 中的 g-NETs 是由其引起的,并推测在 PPI 使用者中具有类似的致瘤作用。为了研究其发病率的增加,g-NETs 已经以多种讨论的方式进行了分类,分为不同的等级,其发病率和明显的发病机制不同。基于大量的实验数据,肿瘤发生是由胃泌素对 ECL 细胞上的 CCK2R 受体的作用介导的,反过来又导致增生、异型增生,最终导致肿瘤发生。然而,在所有三种情况下,ECL 细胞对胃泌素的反应程度都受到许多遗传因素和其他潜在风险因素的影响,以及暴露于激素影响的持续时间的影响。本文回顾了与 PPI 使用引起的高胃泌素血症的营养作用相关的数据,并在附录 A 中总结了所有 11 例在没有 CAG 或 ZES 的情况下发生的长期 PPI 使用者的 g-NETs 报告。还列出了其他地方报告的其他疑似病例。此外,人类的风险可能受到潜在疾病或遗传因素的影响,包括其 PPI 代谢表型,慢代谢者可能面临更高的风险。还讨论了估计 g-NETs 真实发病率的其他问题,涉及到对小肿瘤的漏报以及监测、流行病学和最终结果计划 (SEER) 和其他数据库未能捕获小肿瘤或未给予 T1 评级的问题。总的来说,g-NETs 的真实发病率可能被严重低估:高胃泌素血症是否也会影响胃肠道其他部位或其他器官系统的肿瘤发生的可能性也被简要探讨。总的来说,g-NET 的发病风险在服药超过 10 年且剂量较高的患者中最高:患有慢性胃炎和/或继发胃萎缩的患者也可能面临更高的风险。虽然 PPI 治疗引起的 g-NETs 的总体风险无疑很低,但却是真实存在的:这需要在长期使用 PPI 治疗时谨慎,尤其是在年轻患者中开始使用时。