Duijnhouwer Anthonie, van den Hoven Allard, Merkx Remy, Schokking Michiel, van Kimmenade Roland, Kempers Marlies, Dijk Arie van, de Boer Menko-Jan, Roos-Hesselink Jolien
Department of Cardiology, Radboud university medical center, 6500HB Nijmegen, The Netherlands.
Department of Cardiology, Erasmus medical center, 3000CA Rotterdam, The Netherlands.
J Clin Med. 2020 Jan 21;9(2):290. doi: 10.3390/jcm9020290.
The combination of aortic coarctation (CoA) and bicuspid aortic valve (BAV) is assumed to be associated with a higher risk of ascending aortic dilatation and type A dissection, and current European Society of Cardiology (ESC) guidelines advise therefore to operate at a lower threshold in the presence of CoA. The aim of our study is to evaluate whether the coexistence of CoA in BAV patients is indeed associated with a higher risk of ascending aortic events (AAE).
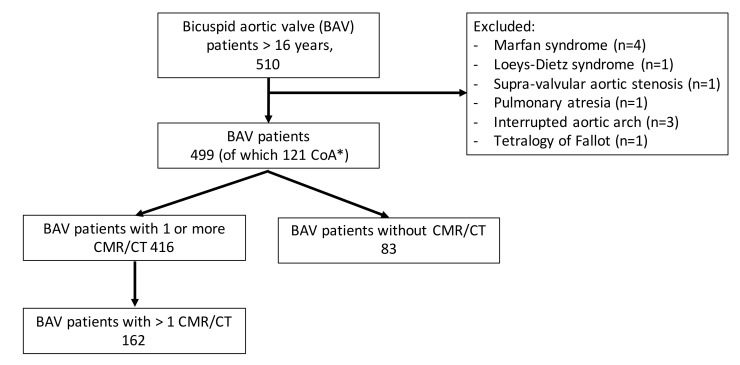
In a retrospective study, all adult BAV patients visiting the outpatient clinic of our tertiary care center between February 2003 and February 2019 were included. The primary end point was an ascending aortic event (AAE) defined as ascending aortic dissection/rupture or preventive surgery. The secondary end points were aortic dilatation and aortic growth.
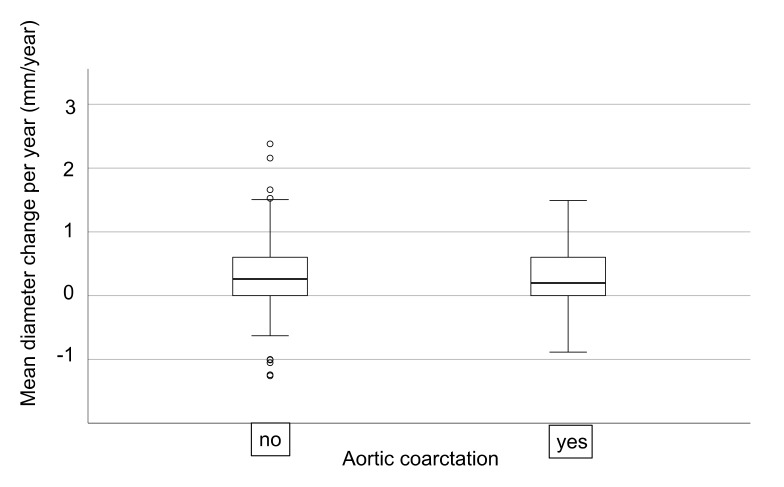
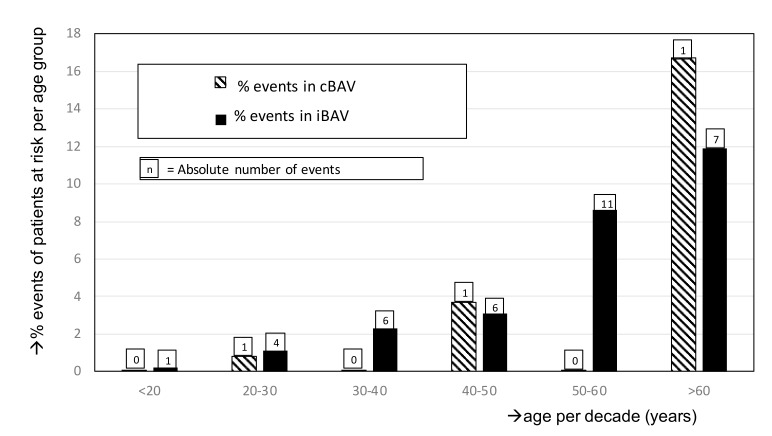
In total, 499 BAV patients (43.7% female, age 40.3 ± 15.7 years) were included, of which 121 (24%) had a history of CoA (cBAV). An aortic event occurred in 38 (7.6%) patients at a mean age of 49.0 ± 13.6 years. In the isolated BAV group (iBAV), significantly more AAE occurred, but this was mainly driven by aortic valve dysfunction as indication for aortic surgery. There was no significant difference in the occurrence of dissection or severely dilated ascending aorta (>50mm) between the iBAV and cBAV patients ( = 0.56). The aortic diameter was significantly smaller in the cBAV group (30.3 ± 6.9 mm versus 35.7 ± 7.6 mm; < 0.001). The median aortic diameter increase was 0.23 (interquartile range (IQR): 0.0-0.67) mm/year and was not significantly different between both groups ( = 0.74).
Coexistence of CoA in BAV patients was not associated with a higher risk of aortic dissection, preventive aortic surgery, aortic dilatation, or more rapid aorta growth. This study suggests that CoA is not a risk factor in BAV patients, and the advice to operate at lower diameter should be reevaluated.
主动脉缩窄(CoA)与二叶式主动脉瓣(BAV)并存被认为与升主动脉扩张和A型主动脉夹层风险较高有关,因此目前欧洲心脏病学会(ESC)指南建议在存在CoA的情况下降低手术阈值。我们研究的目的是评估BAV患者中CoA的并存是否确实与升主动脉事件(AAE)风险较高有关。
在一项回顾性研究中,纳入了2003年2月至2019年2月期间在我们三级医疗中心门诊就诊的所有成年BAV患者。主要终点是升主动脉事件(AAE),定义为升主动脉夹层/破裂或预防性手术。次要终点是主动脉扩张和主动脉生长。
总共纳入了499例BAV患者(女性占43.7%,年龄40.3±15.7岁),其中121例(24%)有CoA病史(cBAV)。38例(7.6%)患者发生主动脉事件,平均年龄为49.0±13.6岁。在单纯BAV组(iBAV)中,发生的AAE明显更多,但这主要是由主动脉瓣功能障碍作为主动脉手术指征所驱动。iBAV和cBAV患者之间在夹层或严重扩张的升主动脉(>50mm)发生率上没有显著差异(P = 0.56)。cBAV组的主动脉直径明显更小(30.3±6.9mm对35.7±7.6mm;P<0.001)。主动脉直径的中位数增加为0.23(四分位间距(IQR):0.0 - 0.67)mm/年,两组之间无显著差异(P = 0.74)。
BAV患者中CoA的并存与主动脉夹层、预防性主动脉手术、主动脉扩张或主动脉更快生长的风险较高无关。本研究表明CoA不是BAV患者的危险因素,应重新评估降低直径阈值进行手术的建议。