Cortellini Alessio, Buti Sebastiano, Bersanelli Melissa, Giusti Raffaele, Perrone Fabiana, Di Marino Pietro, Tinari Nicola, De Tursi Michele, Grassadonia Antonino, Cannita Katia, Tessitore Alessandra, Zoratto Federica, Veltri Enzo, Malorgio Francesco, Russano Marco, Anesi Cecilia, Zeppola Tea, Filetti Marco, Marchetti Paolo, Botticelli Andrea, Cappellini Gian Carlo Antonini, De Galitiis Federica, Vitale Maria Giuseppa, Rastelli Francesca, Pergolesi Federica, Berardi Rossana, Rinaldi Silvia, Tudini Marianna, Silva Rosa Rita, Pireddu Annagrazia, Atzori Francesco, Iacono Daniela, Migliorino Maria Rita, Gelibter Alain, Occhipinti Mario Alberto, Martella Francesco, Inno Alessandro, Gori Stefania, Bracarda Sergio, Zannori Cristina, Mosillo Claudia, Parisi Alessandro, Porzio Giampiero, Mallardo Domenico, Fargnoli Maria Concetta, Tiseo Marcello, Santini Daniele, Ascierto Paolo A, Ficorella Corrado
Medical Oncology, St. Salvatore Hospital, L'Aquila, Italy.
Department of Biotechnological and Applied Clinical Sciences, University of L'Aquila, L'Aquila, Italy.
Oncoimmunology. 2020 Jan 7;9(1):1710389. doi: 10.1080/2162402X.2019.1710389. eCollection 2020.
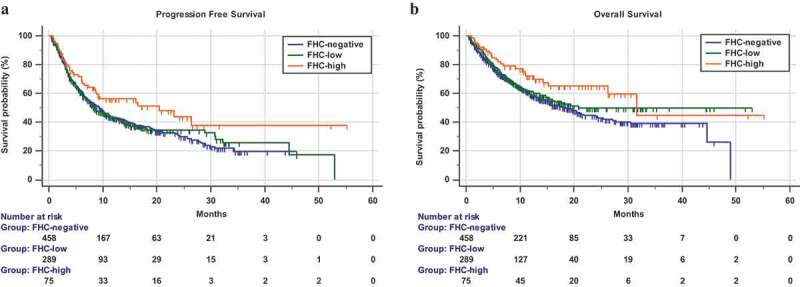
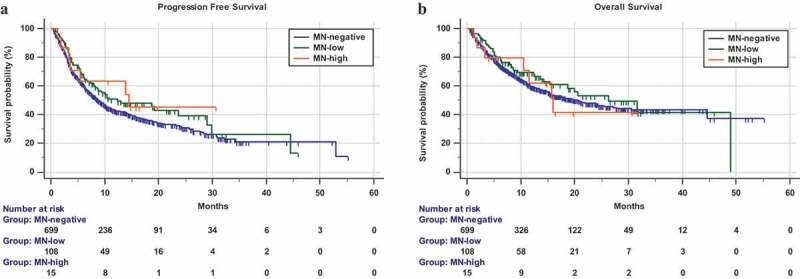
: We investigate the role of family history of cancer (FHC) and diagnosis of metachronous and/or synchronous multiple neoplasms (MN), during anti-PD-1/PD-L1 immunotherapy. : This was a multicenter retrospective study of advanced cancer patients treated with anti-PD-1/PD-L1 immunotherapy. FHC was collected in lineal and collateral lines, and patients were categorized as follows: FHC-high (in case of cancer diagnoses in both the lineal and collateral family lines), FHC-low (in case of cancer diagnoses in only one family line), and FHC-negative. Patients were also categorized according to the diagnosis of MN as follows: MN-high (>2 malignancies), MN-low (two malignancies), and MN-negative. Objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and incidence of immune-related adverse events (irAEs) of any grade were evaluated. : 822 consecutive patients were evaluated. 458 patients (55.7%) were FHC-negative, 289 (35.2%) were FHC-low, and 75 (9.1%) FHC-high, respectively. 29 (3.5%) had a diagnosis of synchronous MN and 94 (11.4%) of metachronous MN. 108 (13.2%) and 15 (1.8%) patients were MN-low and MN-high, respectively. The median follow-up was 15.6 months. No significant differences were found regarding ORR among subgroups. FHC-high patients had a significantly longer PFS (hazard ratio [HR] = 0.69 [95% CI: 0.48-0.97], = .0379) and OS (HR = 0.61 [95% CI: 0.39-0.93], = .0210), when compared to FHC-negative patients. FHC-high was confirmed as an independent predictor for PFS and OS at multivariate analysis. No significant differences were found according to MN categories. FHC-high patients had a significantly higher incidence of irAEs of any grade, compared to FHC-negative patients ( = .0012). : FHC-high patients seem to benefit more than FHC-negative patients from anti-PD-1/PD-L1 checkpoint inhibitors.
我们研究了癌症家族史(FHC)以及异时性和/或同时性多发肿瘤(MN)的诊断在抗PD-1/PD-L1免疫治疗中的作用。
这是一项针对接受抗PD-1/PD-L1免疫治疗的晚期癌症患者的多中心回顾性研究。收集直系和旁系亲属的FHC,并将患者分类如下:FHC高(直系和旁系家族系中均有癌症诊断)、FHC低(仅在一个家族系中有癌症诊断)和FHC阴性。患者还根据MN的诊断分类如下:MN高(>2种恶性肿瘤)、MN低(2种恶性肿瘤)和MN阴性。评估客观缓解率(ORR)、无进展生存期(PFS)、总生存期(OS)以及任何级别的免疫相关不良事件(irAE)的发生率。
对822例连续患者进行了评估。458例患者(55.7%)为FHC阴性,289例(35.2%)为FHC低,75例(9.1%)为FHC高。29例(3.5%)诊断为同时性MN,94例(11.4%)为异时性MN。108例(13.2%)和15例(1.8%)患者分别为MN低和MN高。中位随访时间为15.6个月。各亚组之间在ORR方面未发现显著差异。与FHC阴性患者相比,FHC高的患者PFS显著更长(风险比[HR]=0.69[95%CI:0.48-0.97],P=.0379),OS也显著更长(HR=0.61[95%CI:0.39-0.93],P=.0210)。在多变量分析中,FHC高被确认为PFS和OS的独立预测因素。根据MN类别未发现显著差异。与FHC阴性患者相比,FHC高的患者任何级别的irAE发生率显著更高(P=.0012)。
FHC高的患者似乎比FHC阴性的患者从抗PD-1/PD-L1检查点抑制剂中获益更多。