Department of Radiation Oncology, Shandong Cancer Hospital Affiliated to Shandong University, Jinan, China.
Department of Oncology, Laiwu Central Hospital of Xinwen Mining Group, Jinan, China.
Cancer Res Treat. 2020 Apr;52(2):586-593. doi: 10.4143/crt.2019.242. Epub 2019 Dec 12.
Fractionated radiotherapy as well as concomitant and adjuvant chemotherapy such as temozolomide for postoperative high-grade glioma (HGG) patients improves progression-free survival and overall survival. Multiple factors such as chemotherapy, radiotherapy, tumor grade, residual tumor volume, and genetic modifications might play a role in the formation of cognitive impairment. The risk factors of cognitive impairment in postoperative patients with HGG receiving radiotherapy and chemotherapy remains a concern in this population. The purpose of this study was to identify risk factors for cognitive impairment in patients of postoperative HGG.
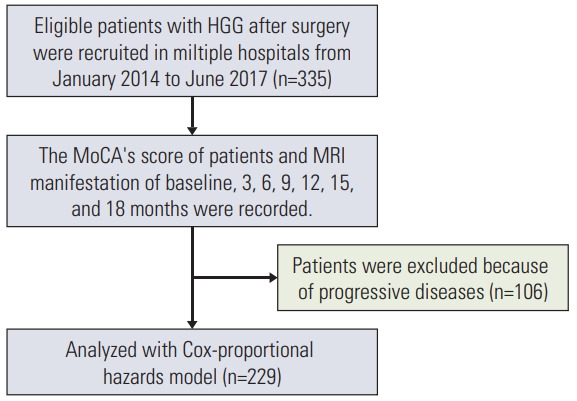
A total of 229 patients with HGG who underwent surgery were analyzed. Cognitive impairment was defined as a decrease of Cognitive Assessment Montreal (MoCA)'s score in at least two cognitive domains or any MoCA's score of less than 26 points at the time of study compared with baseline level. Multiple potential risk factors including methylated status of the O6-methylguanine-DNA methyltransferase (MGMT) promoter, glioma World Health Organization (WHO) grade, residual tumor volume, education, and sex were analyzed. Cox univariate and multivariate regression analysis was used to detect the significant risk factors for cognitive impairment.
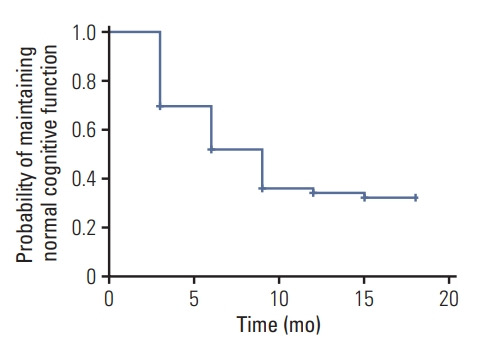
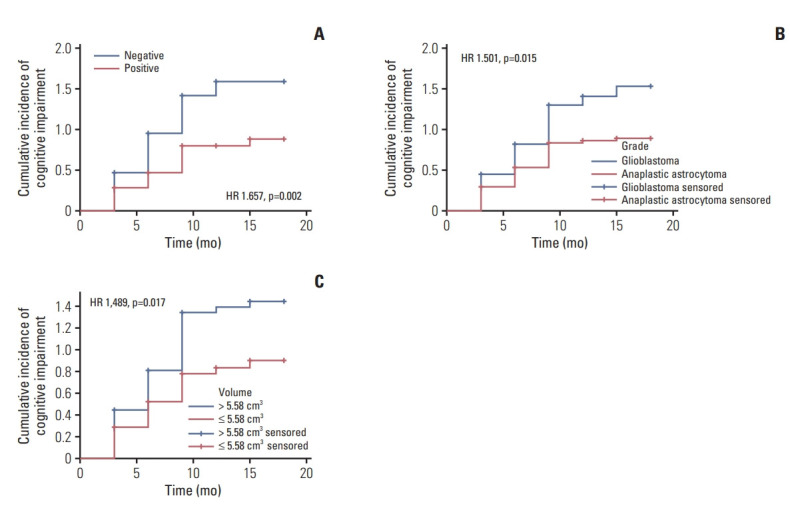
At the end of follow-up among the 229 patients, 147 patients (67%) developed cognitive impairment. 82 patients (36%) remained in normal cognitive condition. In multivariate analysis, unmethylated MGMT promoter (hazard ratio [HR], 1.679; 95% confidence interval [CI], 1.212 to 2.326; p=0.002), glioblastoma (HR, 1.550; 95% CI, 1.117 to 2.149; p=0.009), and residual tumor volume > 5.58 cm3 (HR, 1.454; 95% CI, 1.047 to 2.020; p=0.026) were independent risk factors for cognitive impairment.
Methylated status of the MGMT promoter, glioma WHO grade, and residual tumor volume might be risk factors for the cognitive impairment in postoperative patients with HGG.
术后高级别胶质瘤(HGG)患者接受分割放疗以及替莫唑胺同步和辅助化疗可改善无进展生存期和总生存期。化疗、放疗、肿瘤分级、残余肿瘤体积和遗传修饰等多种因素可能在认知障碍形成中发挥作用。在接受放化疗的术后 HGG 患者中,认知障碍的危险因素仍然是该人群关注的问题。本研究的目的是确定术后 HGG 患者认知障碍的危险因素。
共分析了 229 例接受手术的 HGG 患者。认知障碍定义为与基线相比,研究时认知蒙特利尔认知评估(MoCA)评分至少在两个认知域下降或任何 MoCA 评分低于 26 分。分析了多个潜在的危险因素,包括 O6-甲基鸟嘌呤-DNA 甲基转移酶(MGMT)启动子的甲基化状态、胶质瘤世界卫生组织(WHO)分级、残余肿瘤体积、教育和性别。采用 Cox 单因素和多因素回归分析检测认知障碍的显著危险因素。
在 229 例患者的随访结束时,147 例(67%)发生认知障碍。82 例(36%)患者仍处于正常认知状态。多因素分析显示,未甲基化 MGMT 启动子(危险比[HR],1.679;95%置信区间[CI],1.212 至 2.326;p=0.002)、胶质母细胞瘤(HR,1.550;95%CI,1.117 至 2.149;p=0.009)和残余肿瘤体积>5.58cm3(HR,1.454;95%CI,1.047 至 2.020;p=0.026)是认知障碍的独立危险因素。
MGMT 启动子甲基化状态、胶质瘤 WHO 分级和残余肿瘤体积可能是术后 HGG 患者认知障碍的危险因素。