MMWR Morb Mortal Wkly Rep. 2020 Feb 14;69(6):166-170. doi: 10.15585/mmwr.mm6906e1.
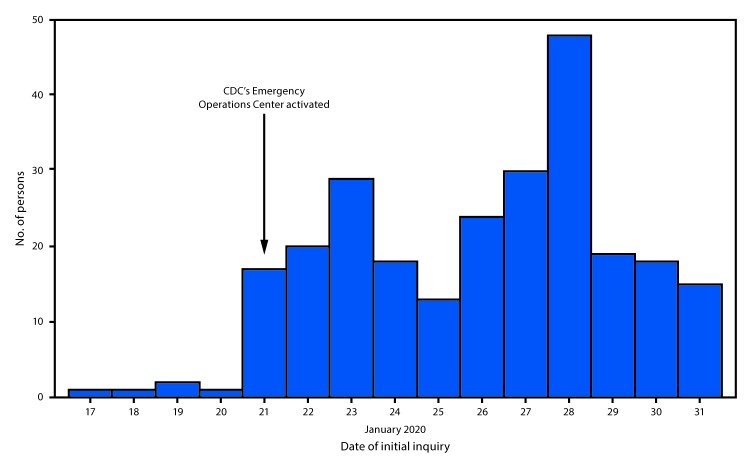
In December 2019, a cluster of cases of pneumonia emerged in Wuhan City in central China's Hubei Province. Genetic sequencing of isolates obtained from patients with pneumonia identified a novel coronavirus (2019-nCoV) as the etiology (1). As of February 4, 2020, approximately 20,000 confirmed cases had been identified in China and an additional 159 confirmed cases in 23 other countries, including 11 in the United States (2,3). On January 17, CDC and the U.S. Department of Homeland Security's Customs and Border Protection began health screenings at U.S. airports to identify ill travelers returning from Wuhan City (4). CDC activated its Emergency Operations Center on January 21 and formalized a process for inquiries regarding persons suspected of having 2019-nCoV infection (2). As of January 31, 2020, CDC had responded to clinical inquiries from public health officials and health care providers to assist in evaluating approximately 650 persons thought to be at risk for 2019-nCoV infection. Guided by CDC criteria for the evaluation of persons under investigation (PUIs) (5), 210 symptomatic persons were tested for 2019-nCoV; among these persons, 148 (70%) had travel-related risk only, 42 (20%) had close contact with an ill laboratory-confirmed 2019-nCoV patient or PUI, and 18 (9%) had both travel- and contact-related risks. Eleven of these persons had laboratory-confirmed 2019-nCoV infection. Recognizing persons at risk for 2019-nCoV is critical to identifying cases and preventing further transmission. Health care providers should remain vigilant and adhere to recommended infection prevention and control practices when evaluating patients for possible 2019-nCoV infection (6). Providers should consult with their local and state health departments when assessing not only ill travelers from 2019-nCoV-affected countries but also ill persons who have been in close contact with patients with laboratory-confirmed 2019-nCoV infection in the United States.
2019 年 12 月,中国中部湖北省武汉市出现了一组肺炎病例。对从肺炎患者中分离出的样本进行基因测序,确定了一种新型冠状病毒(2019-nCoV)为病因(1)。截至 2020 年 2 月 4 日,中国已确诊约 2 万例病例,另有 23 个国家确诊 159 例病例,其中美国 11 例(2,3)。1 月 17 日,美国疾病控制与预防中心(CDC)和美国国土安全部的海关与边境保护局开始在美国机场对入境旅客进行健康筛查,以识别来自武汉市的患病旅客(4)。CDC 于 1 月 21 日启动应急行动中心,并正式制定了询问疑似感染 2019-nCoV 人员的流程(2)。截至 2020 年 1 月 31 日,CDC 已对公共卫生官员和医疗保健提供者提出的临床询问做出回应,以协助评估约 650 名被认为有感染 2019-nCoV 风险的人员。根据 CDC 对调查对象(PUI)评估的标准(5),对 210 名有症状者进行了 2019-nCoV 检测;在这些人中,148 人(70%)只有旅行相关风险,42 人(20%)与确诊的实验室确认的 2019-nCoV 患者或 PUI 有密切接触,18 人(9%)同时具有旅行和接触相关风险。其中 11 人实验室确认感染 2019-nCoV。识别有感染 2019-nCoV 风险的人员对于识别病例和防止进一步传播至关重要。当评估可能感染 2019-nCoV 的患者时,医疗保健提供者应保持警惕并遵守建议的感染预防和控制措施(6)。当评估不仅来自受 2019-nCoV 影响国家的患病旅行者,而且评估与美国实验室确诊的 2019-nCoV 感染患者有密切接触的患病者时,提供者应咨询当地和州卫生部门。