Sonmez Alper, Tasci Ilker, Demirci Ibrahim, Haymana Cem, Barcin Cem, Aydin Hasan, Cetinkalp Sevki, Ozturk Feyza Yener, Gul Kamile, Sabuncu Tevfik, Satman Ilhan, Bayram Fahri
Department of Endocrinology and Metabolism, Gulhane School of Medicine, University of Health Sciences, Ankara, Turkey.
Department of Internal Medicine, Gulhane School of Medicine, University of Health Sciences, Ankara, Turkey.
Diabetes Ther. 2020 May;11(5):1045-1059. doi: 10.1007/s13300-020-00779-0. Epub 2020 Feb 22.
Targeting better glycated hemoglobin (HbA1c) and blood pressure (BP) goals may endanger older adults with type 2 diabetes mellitus (T2DM). Overtreatment of T2DM and hypertension is a trending issue, although undertreatment is still common. We investigated the rates and predictors of overtreatment and undertreatment of glycemia and BP in older adults with T2DM and physicians' attitudes to deintensify or intensify treatment.
Data from older adults (≥ 65 years) enrolled in a large nationwide T2DM survey in 2017 across Turkey were analyzed. Overtreatment of glycemia was defined as HbA1c < 6.5% plus the use of ≥ 2 oral antihyperglycemics or insulin, and BP overtreatment was defined as systolic BP (SBP) < 120 mmHg or diastolic BP (DBP) < 65 mmHg plus the use of ≥ 2 drugs. Undertreatment of glycemia was defined as HbA1c > 9%, and BP undertreatment was defined as SBP > 150 mmHg or DBP > 90 mmHg. Deintensification or intensification rates were calculated according to treatment modification initiated by the treating physician(s).
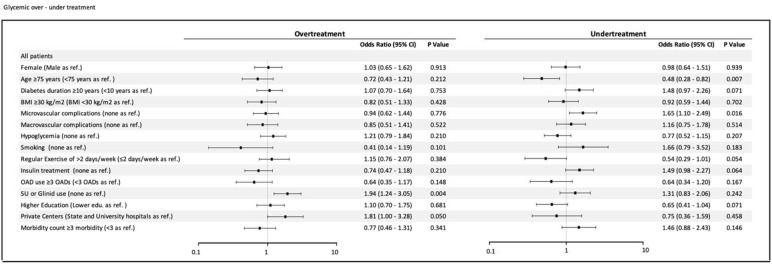
The rate of overtreatment in the glycemia group (n = 1264) was 9.8% (n = 124) and that in the BP group (n = 1052) was 7.3% (n = 77), whereas the rate of undertreatment was 14.2% (n = 180) and 15.2% (n = 160), respectively. In the adjusted model, use of oral secretagogues (sulfonylureas or glinides) (odds ratio [OR] 1.94, 95% confidence interval [CI] 1.2-3.1) and follow-up at a private clinic (OR 1.81, 95% CI 1.0-3.3) were predictors of glycemia overtreatment. BP overtreatment was independently associated with the use insulin-based diabetes therapies (OR 1.86, 95% CI 1.14-3.04). There was no independent association of BP undertreatment to the study confounders. The deintensification and intensification rates were 25 and 75.6%, respectively, for glycemia and 10.9 and 9.2%, respectively, for BP.
The results show that one in ten older adults with T2DM are overtreated while one in four require modification of their current antihyperglycemic and antihypertensive treatments. Physicians are eager to intensify medications while they largely ignore deintensification in diabetes management. These results warrant enforced measures to improve the care of older adults with T2DM.
ClinicalTrials.gov identifier, NCT03455101.
追求更好的糖化血红蛋白(HbA1c)和血压(BP)目标可能会危及老年2型糖尿病(T2DM)患者。T2DM和高血压的过度治疗是一个热门问题,尽管治疗不足仍然很常见。我们调查了老年T2DM患者血糖和血压过度治疗与治疗不足的发生率及预测因素,以及医生对强化或弱化治疗的态度。
分析了2017年土耳其全国范围内一项大型T2DM调查中纳入的老年(≥65岁)患者的数据。血糖过度治疗定义为HbA1c<6.5%且使用≥2种口服降糖药或胰岛素,血压过度治疗定义为收缩压(SBP)<120 mmHg或舒张压(DBP)<65 mmHg且使用≥2种药物。血糖治疗不足定义为HbA1c>9%,血压治疗不足定义为SBP>150 mmHg或DBP>90 mmHg。根据治疗医生发起的治疗调整计算弱化或强化率。
血糖组(n = 1264)的过度治疗率为9.8%(n = 124),血压组(n = 1052)为7.3%(n = 77),而治疗不足率分别为14.2%(n = 180)和15.2%(n = 160)。在调整模型中,使用口服促分泌剂(磺脲类或格列奈类)(比值比[OR]1.94,95%置信区间[CI]1.2 - 3.1)和在私人诊所随访(OR 1.81,95%CI 1.0 - 3.3)是血糖过度治疗的预测因素。血压过度治疗与使用胰岛素类糖尿病治疗独立相关(OR 1.86,95%CI 1.14 - 3.04)。血压治疗不足与研究混杂因素无独立关联。血糖的弱化和强化率分别为25%和75.6%,血压分别为10.9%和9.2%。
结果表明,每10名老年T2DM患者中就有1名接受了过度治疗,而每4名患者中就有1名需要调整其目前的降糖和降压治疗。医生急于强化药物治疗,而在糖尿病管理中很大程度上忽视了弱化治疗。这些结果需要采取强制措施来改善老年T2DM患者的护理。
ClinicalTrials.gov标识符,NCT03455101。