Botero Juliana Perez, Lee Kristy, Branchford Brian R, Bray Paul F, Freson Kathleen, Lambert Michele P, Luo Minjie, Mohan Shruthi, Ross Justyne E, Bergmeier Wolfgang, Di Paola Jorge
Versiti and Division of Hematology/Oncology, Medical College of Wisconsin, Milwaukee, WI, USA.
Department of Genetics, University of North Carolina at Chapel Hill, NC, USA.
Haematologica. 2020 Apr;105(4):888-894. doi: 10.3324/haematol.2018.214239. Epub 2020 Mar 5.
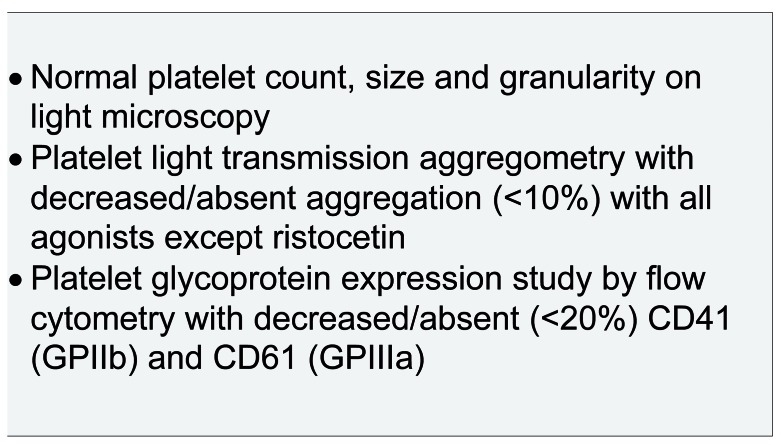
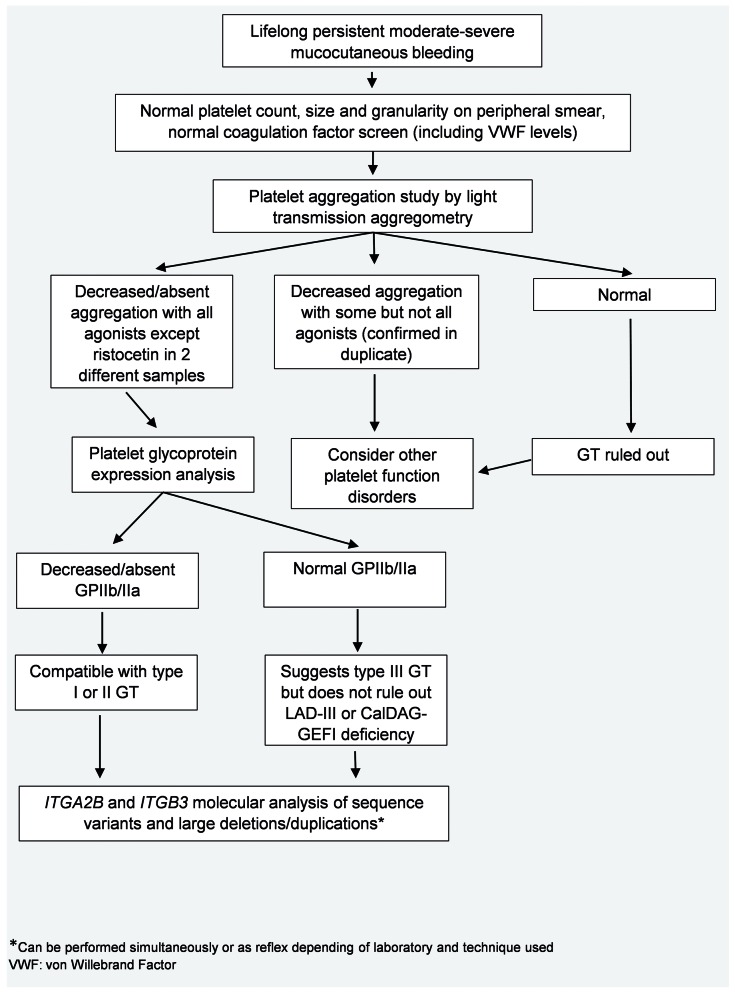
Glanzmann thrombasthenia (GT) is an autosomal recessive disorder of platelet aggregation caused by quantitative or qualitative defects in integrins αIIb and β3. These integrins are encoded by the and genes and form platelet glycoprotein (GP)IIb/IIIa, which acts as the principal platelet receptor for fibrinogen. Although there is variability in the clinical phenotype, most patients present with severe mucocutaneous bleeding at an early age. A classic pattern of abnormal platelet aggregation, platelet glycoprotein expression and molecular studies confirm the diagnosis. Management of bleeding is based on a combination of hemostatic agents including recombinant activated factor VII with or without platelet transfusions and antifibrinolytic agents. Refractory bleeding and platelet alloimmunization are common complications. In addition, pregnant patients pose unique management challenges. This review highlights clinical and molecular aspects in the approach to patients with GT, with particular emphasis on the significance of multidisciplinary care.
血小板无力症(GT)是一种常染色体隐性血小板聚集障碍疾病,由整合素αIIb和β3的数量或质量缺陷引起。这些整合素由 和 基因编码,形成血小板糖蛋白(GP)IIb/IIIa,它是纤维蛋白原的主要血小板受体。尽管临床表型存在差异,但大多数患者在幼年时就出现严重的黏膜皮肤出血。异常血小板聚集、血小板糖蛋白表达和分子研究的经典模式可确诊。出血的治疗基于多种止血药物的联合使用,包括重组活化因子VII(有或无血小板输注)和抗纤溶药物。难治性出血和血小板同种免疫是常见并发症。此外,妊娠患者带来独特的管理挑战。本综述强调了GT患者治疗中的临床和分子方面,特别强调多学科护理的重要性。