Montfort Research Institute, 713 Montreal Road, Ottawa, Canada.
Ottawa Hospital Research Institute, 501 Smyth Road, Ottawa, K1H 8L6, Canada.
Syst Rev. 2020 Mar 9;9(1):53. doi: 10.1186/s13643-020-01305-w.
As systematic reviews' limited coverage of the medical literature necessitates decision-making based on unsystematic review, we investigated a possible advantage of systematic review (aside from dataset size and systematic analysis): does systematic review avoid potential bias in sampling primary studies from high impact factor journals? If randomized controlled trials (RCTs) reported in higher-impact journals present different treatment benefits than RCTs reported in lower-impact journals, readers who focus on higher-impact journals for their rapid literature reviews may introduce bias which could be mitigated by complete, systematic sampling.
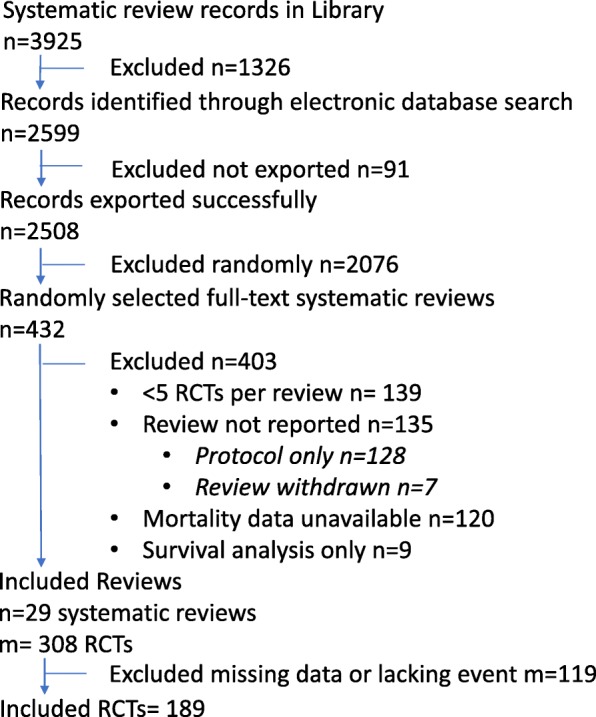
We randomly sampled Cochrane Library (20 July 2005) treatment reviews that measured mortality as a binary outcome, published in English or French, with at least five RCTs with one or more deaths. Our domain-based assessment of risk of bias included funding source, randomness of allocation sequence, blinding, and allocation concealment. The primary analysis employed logistic regression by a generalized linear model with a generalized estimating equation to estimate the association between various factors and publication in a journal with a high journal impact factor (JIF).
From the 29 included systematic reviews, 189 RCTs contributed data. However, in the primary analyses comparing RCT results within meta-analyses, there was no statistically significant association: unadjusted odds of greater than 50% mortality protection in high-JIF (> 5) journals were 1.4 (95% CI 0.42, 4.4) and adjusted, 2.5 (95% CI 0.6, 10). Elements of study quality were weakly, inconsistently, and not statistically significantly correlated with journal impact factor.
Journal impact factor may have little to no association with study results, or methodological quality, but the evidence is very uncertain.
由于系统评价对医学文献的覆盖有限,因此需要基于非系统评价做出决策,我们研究了系统评价可能具有的一个优势(除了数据集的大小和系统分析之外):系统评价是否可以避免从高影响因子期刊中选择原始研究时的潜在偏倚?如果在高影响因子期刊中报告的随机对照试验(RCT)与在低影响因子期刊中报告的 RCT 相比具有不同的治疗效果,那么那些为了快速文献综述而专注于高影响因子期刊的读者可能会引入偏倚,而通过全面、系统的抽样可以减轻这种偏倚。
我们随机抽取了 Cochrane Library(2005 年 7 月 20 日)中以死亡率为二分类结局的治疗评价,发表于英文或法文,至少包含 5 项有 1 个或多个死亡的 RCT。我们基于领域的偏倚风险评估包括了资金来源、分配序列的随机性、盲法和分配隐藏。主要分析采用了广义线性模型的逻辑回归,通过广义估计方程来估计各种因素与发表在高期刊影响因子(JIF)期刊之间的关联。
在 29 项纳入的系统评价中,有 189 项 RCT 提供了数据。然而,在对各亚组分析中比较 RCT 结果时,并没有统计学上的显著关联:高 JIF(>5)期刊中大于 50%的死亡率保护的未调整比值比为 1.4(95%CI 0.42, 4.4),调整后的比值比为 2.5(95%CI 0.6, 10)。研究质量的各个要素与期刊影响因子之间存在微弱、不一致且无统计学意义的相关性。
期刊影响因子可能与研究结果或方法学质量几乎没有关联,但证据非常不确定。