Mid-Atlantic Epilepsy and Sleep Center, Bethesda, Maryland.
Departments of Physiology and Cell Biology, and Brain and Cognitive Science, Zlotowski Center for Neuroscience, Ben-Gurion University of the Negev, Beer-Sheva, Israel.
Epilepsia. 2020 Mar;61(3):359-386. doi: 10.1111/epi.16450.
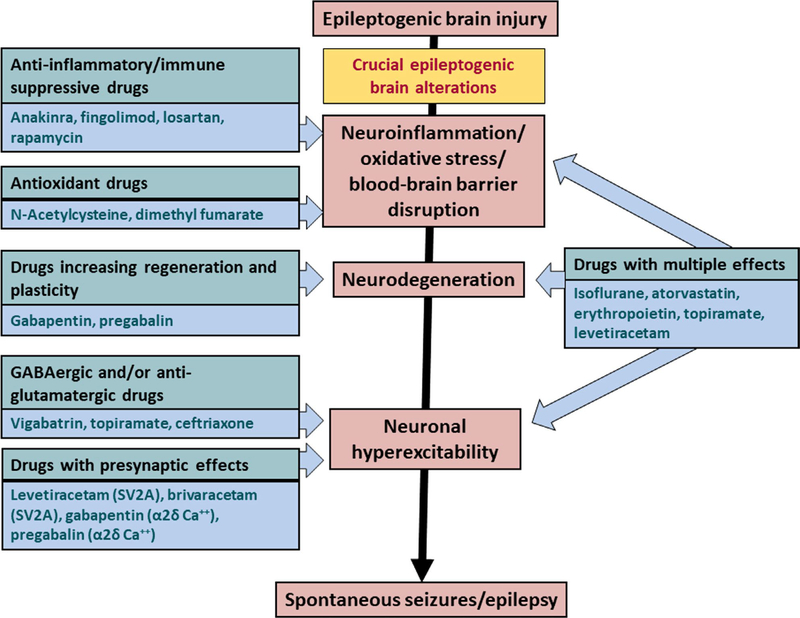
Prevention of epilepsy is a great unmet need. Acute central nervous system (CNS) insults such as traumatic brain injury (TBI), cerebrovascular accidents (CVA), and CNS infections account for 15%-20% of all epilepsy. Following TBI and CVA, there is a latency of days to years before epilepsy develops. This allows treatment to prevent or modify postinjury epilepsy. No such treatment exists. In animal models of acquired epilepsy, a number of medications in clinical use for diverse indications have been shown to have antiepileptogenic or disease-modifying effects, including medications with excellent side effect profiles. These include atorvastatin, ceftriaxone, losartan, isoflurane, N-acetylcysteine, and the antiseizure medications levetiracetam, brivaracetam, topiramate, gabapentin, pregabalin, vigabatrin, and eslicarbazepine acetate. In addition, there are preclinical antiepileptogenic data for anakinra, rapamycin, fingolimod, and erythropoietin, although these medications have potential for more serious side effects. However, except for vigabatrin, there have been almost no translation studies to prevent or modify epilepsy using these potentially "repurposable" medications. We may be missing an opportunity to develop preventive treatment for epilepsy by not evaluating these medications clinically. One reason for the lack of translation studies is that the preclinical data for most of these medications are disparate in terms of types of injury, models within different injury type, dosing, injury-treatment initiation latencies, treatment duration, and epilepsy outcome evaluation mode and duration. This makes it difficult to compare the relative strength of antiepileptogenic evidence across the molecules, and difficult to determine which drug(s) would be the best to evaluate clinically. Furthermore, most preclinical antiepileptogenic studies lack information needed for translation, such as dose-blood level relationship, brain target engagement, and dose-response, and many use treatment parameters that cannot be applied clinically, for example, treatment initiation before or at the time of injury and dosing higher than tolerated human equivalent dosing. Here, we review animal and human antiepileptogenic evidence for these medications. We highlight the gaps in our knowledge for each molecule that need to be filled in order to consider clinical translation, and we suggest a platform of preclinical antiepileptogenesis evaluation of potentially repurposable molecules or their combinations going forward.
预防癫痫是一个巨大的未满足需求。急性中枢神经系统(CNS)损伤,如创伤性脑损伤(TBI)、脑血管意外(CVA)和 CNS 感染,占所有癫痫的 15%-20%。TBI 和 CVA 后,癫痫发作有几天到几年的潜伏期。这使得治疗可以预防或改变损伤后的癫痫。目前尚无此类治疗方法。在获得性癫痫的动物模型中,许多用于多种适应证的临床用药已被证明具有抗癫痫或疾病修饰作用,包括具有良好副作用谱的药物。这些药物包括阿托伐他汀、头孢曲松、氯沙坦、异氟烷、N-乙酰半胱氨酸和抗癫痫药物左乙拉西坦、布瓦西坦、托吡酯、加巴喷丁、普瑞巴林、vigabatrin 和 eslicarbazepine 醋酸盐。此外,还有用于白介素-1 受体拮抗剂、雷帕霉素、芬戈莫德和促红细胞生成素的临床前抗癫痫发生数据,尽管这些药物可能有更严重的副作用。然而,除了 vigabatrin 之外,几乎没有使用这些潜在的“可再利用”药物来预防或改变癫痫的翻译研究。我们可能会错过开发癫痫预防治疗的机会,因为我们没有对这些药物进行临床评估。缺乏翻译研究的一个原因是,大多数这些药物的临床前数据在损伤类型、不同损伤类型内的模型、剂量、损伤-治疗开始潜伏期、治疗持续时间以及癫痫结果评估模式和持续时间方面存在差异。这使得比较这些分子的抗癫痫发生证据的相对强度变得困难,也难以确定哪种药物(或多种药物)最适合临床评估。此外,大多数临床前抗癫痫发生研究缺乏翻译所需的信息,例如剂量-血药浓度关系、大脑靶标结合和剂量反应,并且许多研究使用无法在临床上应用的治疗参数,例如在损伤前或损伤时开始治疗以及给药剂量高于人类等效剂量耐受。在这里,我们综述了这些药物的动物和人类抗癫痫发生证据。我们强调了每个分子都需要填补的知识空白,以便考虑临床转化,并且我们建议在未来建立一个潜在可再利用分子或其组合的临床前抗癫痫发生评估平台。