Joshi Nikhil V, Elkhawad Maysoon, Forsythe Rachael O, McBride Olivia M B, Rajani Nikil K, Tarkin Jason M, Chowdhury Mohammed M, Donoghue Emma, Robson Jennifer M J, Boyle Jonathan R, Fryer Tim D, Huang Yuan, Teng Zhongzhao, Dweck Marc R, Tawakol Ahmed A, Gillard Jonathan H, Coughlin Patrick A, Wilkinson Ian B, Newby David E, Rudd James H F
Centre for Cardiovascular Science, University of Edinburgh, Edinburgh, UK.
Division of Cardiovascular Medicine, University of Cambridge, Cambridge, UK.
Open Heart. 2020 Mar 11;7(1):e001141. doi: 10.1136/openhrt-2019-001141. eCollection 2020.
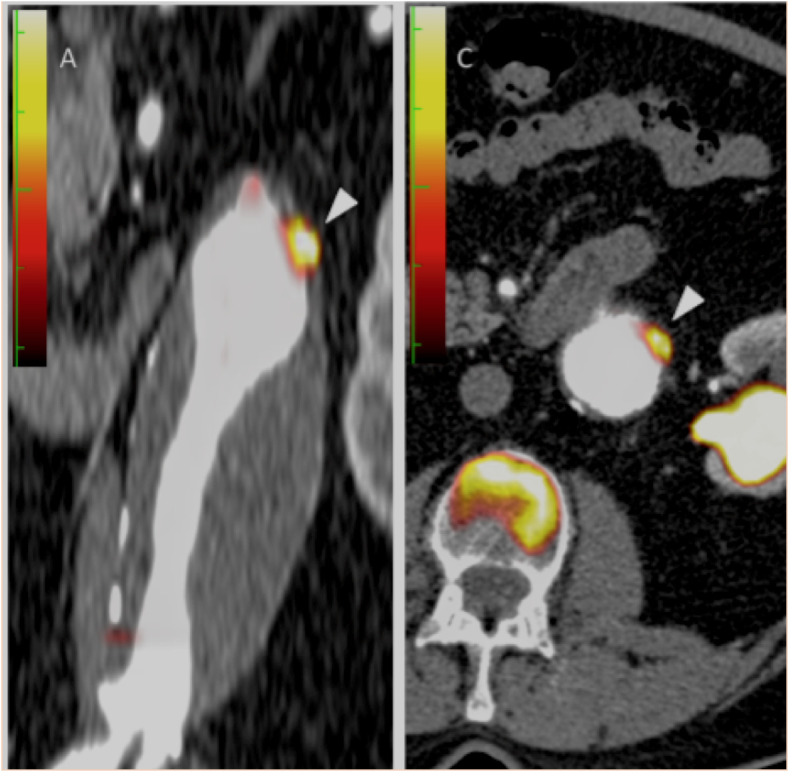
Using combined positron emission tomography and CT (PET-CT), we measured aortic inflammation and calcification in patients with abdominal aortic aneurysms (AAA), and compared them with matched controls with atherosclerosis.
We prospectively recruited 63 patients (mean age 76.1±6.8 years) with asymptomatic aneurysm disease (mean size 4.33±0.73 cm) and 19 age-and-sex-matched patients with confirmed atherosclerosis but no aneurysm. Inflammation and calcification were assessed using combined 18F-FDG PET-CT and quantified using tissue-to-background ratios (TBRs) and Agatston scores.
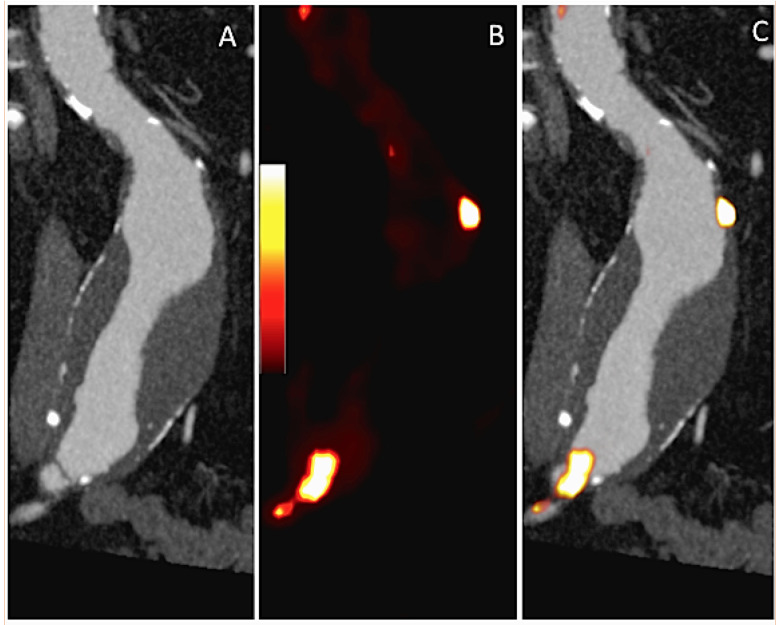
In patients with AAA, 18F-FDG uptake was higher within the aneurysm than in other regions of the aorta (mean TBR2.23±0.46 vs 2.12±0.46, p=0.02). Compared with atherosclerotic control subjects, both aneurysmal and non-aneurysmal aortae showed higher 18F-FDG accumulation (total aorta mean TBR2.16±0.51 vs 1.70±0.22, p=0.001; AAA mean TBR2.23±0.45 vs 1.68±0.21, p<0.0001). Aneurysms containing intraluminal thrombus demonstrated lower 18F-FDG uptake within their walls than those without (mean TBR2.14±0.43 vs 2.43±0.45, p=0.018), with thrombus itself showing low tracer uptake (mean TBR thrombus 1.30±0.48 vs aneurysm wall 2.23±0.46, p<0.0001). Calcification in the aneurysmal segment was higher than both non-aneurysmal segments in patients with aneurysm (Agatston 4918 (2901-8008) vs 1017 (139-2226), p<0.0001) and equivalent regions in control patients (442 (304-920) vs 166 (80-374) Agatston units per cm, p=0.0042).
The entire aorta is more inflamed in patients with aneurysm than in those with atherosclerosis, perhaps suggesting a generalised inflammatory aortopathy in patients with aneurysm. Calcification was prominent within the aneurysmal sac, with the remainder of the aorta being relatively spared. The presence of intraluminal thrombus, itself metabolically relatively inert, was associated with lower levels of inflammation in the adjacent aneurysmal wall.
使用正电子发射断层扫描与计算机断层扫描相结合的技术(PET-CT),我们测量了腹主动脉瘤(AAA)患者的主动脉炎症和钙化情况,并将其与匹配的动脉粥样硬化对照组进行比较。
我们前瞻性招募了63例无症状动脉瘤疾病患者(平均年龄76.1±6.8岁,平均瘤体大小4.33±0.73 cm)以及19例年龄和性别匹配、确诊有动脉粥样硬化但无动脉瘤的患者。使用18F-FDG PET-CT联合评估炎症和钙化情况,并使用组织与本底比值(TBR)和阿加斯顿评分进行量化。
在AAA患者中,动脉瘤内18F-FDG摄取高于主动脉其他区域(平均TBR 2.23±0.46 vs 2.12±0.46,p = 0.02)。与动脉粥样硬化对照组相比,动脉瘤和非动脉瘤主动脉的18F-FDG积聚均更高(整个主动脉平均TBR 2.16±0.51 vs 1.70±0.22,p = 0.001;AAA平均TBR 2.23±0.45 vs 1.68±0.21,p < 0.0001)。含有腔内血栓的动脉瘤其壁内18F-FDG摄取低于无血栓的动脉瘤(平均TBR 2.14±0.43 vs 2.43±0.45,p = 0.018),血栓本身示踪剂摄取较低(平均TBR血栓1.30±0.48 vs动脉瘤壁2.23±0.46,p < 0.0001)。动脉瘤节段的钙化高于动脉瘤患者的非动脉瘤节段(阿加斯顿评分4918(2901 - 8008)vs 1017(139 - 2226),p < 0.0001)以及对照组患者的等效区域(每厘米阿加斯顿单位442(304 - 920)vs 166(80 - 374),p = 0.0042)。
动脉瘤患者的整个主动脉炎症程度高于动脉粥样硬化患者,这可能提示动脉瘤患者存在全身性炎症性主动脉病变。钙化在动脉瘤腔内较为突出,主动脉其余部分相对较少。腔内血栓的存在本身代谢相对惰性,与相邻动脉瘤壁较低水平的炎症相关。